
Clinical Competency Committees
A Guidebook for Programs
3
rd
Edition
Kathryn Andolsek
Duke University
Jamie Padmore
Medstar-Georgetown
Karen E. Hauer
University of California at San Francisco
Andem Ekpenyong
Rush University Hospital
Laura Edgar
ACGME
Eric Holmboe
ACGME
This information is current as of January 2020
Overview
The Clinical Competency Committee (CCC) is a structure that has emerged as an
essential component of the evaluation process in graduate medical education
(GME). While some specialties and programs have utilized CCCs for years, this
structure is still relatively new to many others. Likewise, with the emergence of the
CCC as a requirement for accreditation (ACGME Common Program
Requirements), even seasoned programs and committees are facing questions
regarding the CCC’s structure, function, and process. Furthermore, scholarship on
group decision making, assessment, and CCCs themselves continues to provide
evidence to inform practices. The purpose of this manual, now in its third edition, is
to provide designated institutional officials (DIOs), program directors, faculty
members, CCC members, coordinators, residents, and fellows with information and
practical advice regarding the structure, implementation, function, and utility of a
well-functioning CCC. The materials were prepared for both individual learning and
application in a group setting. Ideally, institutions and programs will be able to use
these materials to have meaningful conversations with all stakeholders; enhance
CCC development, function, and outcomes; and improve transparency for residents
and fellows on the nature of assessment in competency-based education. This third
edition also contains updated material and new tools for programs to use to
continually improve their CCC processes, and a section on institutional
opportunities with CCCs has been added. Each major section has an
accompanying brief “summary” available as a separate, individual document.
This manual provides information related to the following topics:
1. Purposes of a CCC
2. CCC Structure and Membership
3. Preparing for CCC meetings
4. Running the CCC meeting, including effective group process
5. Post-meeting feedback, documentation. and follow-up
6. Legal issues
7. Other Uses for the CCC
8. Individualized Learning Plans
9. Institutional Oversight of CCCs
10. Current Research
Several appendices contain tools for institutions, programs, and CCCs. A robust
body of research to support the various aspects of CCCs, including assessment,
feedback, documentation, group dynamics, and outcomes, is now available. An
annotated bibliography is updated approximately every six months and is available
on the Milestones section of the ACGME website.
The ACGME welcomes feedback, and hopes this guidebook provides institutions,
programs, and faculty members with valuable information and tools to enhance
GME.
1
Table of Contents
Sections
Page
1. Introduction
2
2. Purpose of a CCC
5
3. CCC Structure and Membership
8
4. Preparing for CCC meeting
20
5. Running the CCC meeting
26
6. Post-meeting activities
36
7. Legal issues
39
8. Other Uses for the CCC
46
9. Individualized Learning Plans
50
10. Institutional Oversight of CCCs
56
11. Current Research
58
Appendices
Page
A. The High Performing Residency Assessment System
59
B. CCC Quiz
61
C. Case Studies
67
D. Designing the CCC
71
E. Examples of Assessment Methods for the ACGME Core
Competencies
82
F. Overview of Assessment Methods Aligned with Miller’s Pyramid
84
G. PPV (Predictive Probability Value) Tables
85
H. ADAPT Model of Feedback
86
I. R2C2 Evidence-Informed Facilitated Feedback
87
J. Institutional Checklist for CCCs
89
2
Introduction
The Clinical Competency Committee (CCC) became a central tool in graduate
medical education (GME) as the ACGME transitioned to its current model of
accreditation (previously dubbed the “Next Accreditation System”) as an important
element of competency-based education. ACGME International (ACGME-I)
programs use CCCs as well. The requirements for CCCs have evolved with the
most recently revised ACGME Common Program Requirements, effective July 1,
2019. All four sets of Common Program Requirements (Residency; Fellowship;
One-Year Fellowship; and Post-Doctoral Education Programs) have the same
requirements. The ACGME has categorized all requirements for CCCs as “Core”
requirements, meaning they are required for every graduate medical education
program. The requirements are discussed in Part 2 of this guidebook.
The objectives of this guidebook are to help institutions and programs:
1. Recognize the role and purpose of the CCC for individual programs in the
ACGME’s current accreditation model.
2. Design, create, implement, and continuously improve the program’s CCC.
3. Run an effective CCC meeting.
4. Provide feedback to residents or fellows allowing for improved constructed
individual learning plans.
5. Anticipate questions regarding “process” and considerations of academic
law.
6. Align the program’s own CCC processes with the best evidence from the
medical education literature.
7. Use the CCC to continuously improve the program’s curriculum,
assessment system, faculty development, and clinical
training/experiences/quality.
The guidebook also aims to help programs understand other opportunities for using
Milestones data and for designated institutional officials (DIOs) to recognize
opportunities to support CCCs at an institutional level.
This guidebook is intended to be a practical resource and a professional
development tool for institutional and program leadership, coordinator(s), and
faculty members. Residents and fellows may also benefit from this guidebook,
although a separate guidebook has been developed specifically for them:
Milestones Guidebook for Residents and Fellows. Institutional and program leaders
are encouraged to share these materials with their program faculty members and
leaders, and to use the exercises as part of faculty and coordinator professional
development. These materials can be reviewed individually or as part of a meeting.
The guidebook also provides suggestions for faculty development.
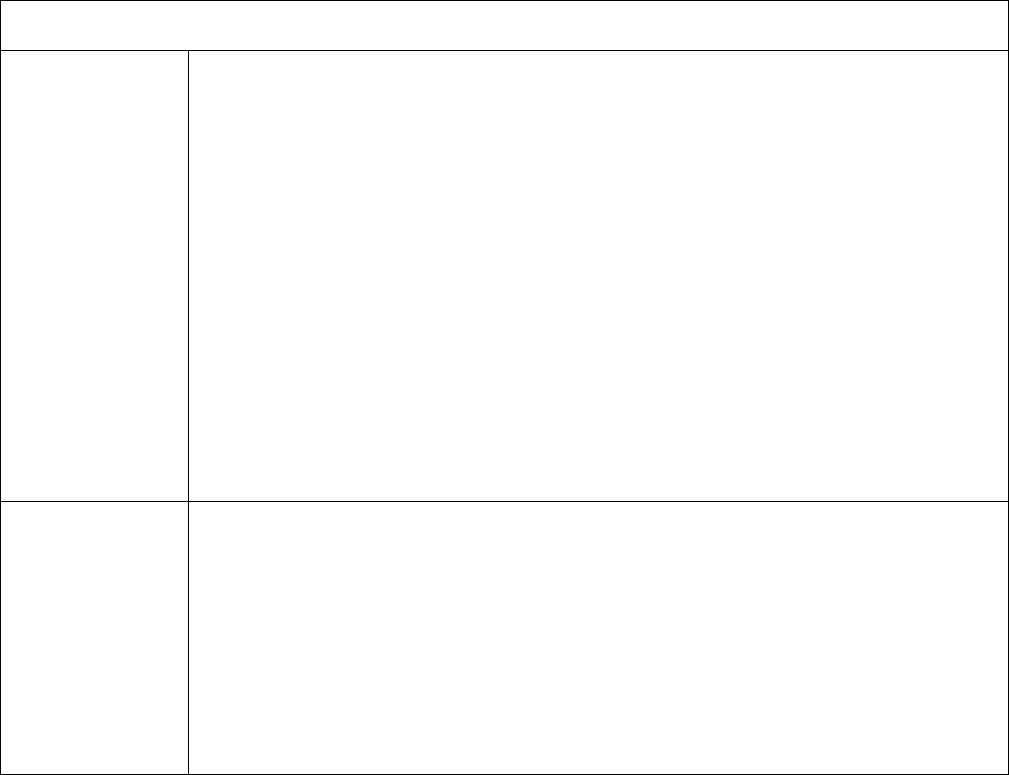
The CCC contributes to an effective resident/fellow assessment system as outlined
in Figure 1. In this figure, the CCC serves the critically important function of
synthesizing multiple quantitative and qualitative assessments regarding individual
resident/fellow performance. This figure highlights several important points:
1. The CCC’s deliberative process will depend on the quality of the assessment
program that should include a combination of assessment methods and a
number of different assessors. Ideally, the individuals who sit on the CCC must

3
understand the basics of good assessment and the assessment tools being
used by the program. Faculty members should have opportunities to enhance
their assessment skills and understand how their assessments fit into the
program’s overall assessment strategy.
2. Residents and fellows are adult learners and must be active agents in this
system; guided self-directed assessment behaviors by an individual resident or
fellow should be expected and strongly cultivated. Programs are urged to
encourage all of their residents and fellows to review the Milestones Guidebook
for Residents and Fellows (available at
http://www.acgme.org/Portals/0/PDFs/Milestones/MilestonesGuidebookforResid
entsFellows.pdf)
3. The program director of a residency, fellowship, or post-graduate educational
program is the ultimate arbiter of whether a resident or fellow is ready to
practice without supervision. The accountability of the program director and
the program cannot be over-emphasized: professional self-regulation depends
heavily on the informed judgment of education programs, as manifest by the
final summative evaluation of competence and entrustment made by the
program director.

4
Figure 1: Structure of a High Performing Resident/Fellow Assessment System
Residents = both residents and fellows
FB = Feedback loops
D = Assessment data and information
The model is more fully described in Appendix A
In this model the Data Synthesis Committee IS the CCC.
Holmboe ES, Yamazaki K, Edgar L, et al. Reflections on the first 2 years of
milestone implementation. J Grad Med Educ. 2015;7(3):506-511.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4597976/
. 2020.
5
Part 1: Purpose of a CCC
The CCC serves several purposes for multiple stakeholders: the program itself,
program directors, faculty members, program coordinators, residents and fellows,
the institution, and the ACGME (Table 1). The ultimate purpose is to demonstrate
accountability as medical educators to the public: that graduates will provide high
quality, safe care to patients while in training, and be well prepared to do so once in
practice.
Table 1: Purposes of a CCC
Purpose of CCC
Program
● Develop shared mental model of what resident/fellow performance should
“look like” and how it should be measured and assessed
● Ensure the right combination of assessment tools to effectively determine
performance across the Competencies and specialty-specific Milestones
● Increase quality, standardize expectations, and reduce variability in
performance assessment
● Contribute to aggregate data that will allow programs to learn from each
other by comparing residents’ and fellows’ judgments against national data
● Improve individual residents’/fellows’ progress along a developmental
trajectory
● Identify early those residents/fellows who are challenged and not making
expected progress so that individualized learning plans can be designed
● Identify advanced residents/fellows to offer them innovative educational
opportunities to further enhance their development
● Identify weaknesses/gaps in the program as a first step in program
improvement
● Model “real time” faculty development
Program
Director
● Fulfill public accountability by ensuring that residents/fellows who
successfully complete a program can practice without supervision
● Engage faculty members, and others when appropriate, to make informed
decisions regarding performance
● Enhance credibility of judgments about resident/fellow performance
● Identify opportunities for faculty development around supervision and
assessment, both formative and summative
● Facilitate the program director’s role as “advocate” for the resident/fellow
● Improve feedback for residents and fellows

6
Table 1 (continued)
Faculty
Members
● Facilitate faculty members’ development of a shared mental model of what
is expected within each of the Competencies and specialty-specific
Milestones
● Improve documentation by simplifying and creating “more actionable” and
efficient assessment tools for the direct observation of residents/fellows in
the clinical learning environment
● Fulfill the professionalism inherent in the faculty member’s role by
contributing high quality teaching and assessment as part of the program
● Contribute accurate, rich descriptive assessment information to the CCC
Program
Coordinators
● Optimize resident/fellow data management systems
● Synthesize assessment data
● Improve methods to share data with the CCC
● Collaborate with program directors to ensure residents and fellows receive
feedback and follow-up, and that Milestones assessments are reported to
the ACGME
● Help improve CCC process by observing the meeting dynamics and
providing feedback
Residents/
Fellows
● Improve the quality, amount, and timing of feedback; normalize
constructive feedback
● Offer insights and perspectives of a group of faculty members
● Enhance self-directed learning
● Compare performance against established Competency benchmarks
(rather than only against peers in the same program)
● Allow earlier identification of sub-optimal performance that can inform
individualized learning plans and improve individualized interventions
● Improve “stretch goals” for residents/fellows to help high performing
residents/fellows achieve even greater competence
● Provide transparency regarding performance expectations
Institutions
● Ensure residents/fellows are making expected progress and those who are
not are provided an opportunity for early intervention
● Provide foundational expectations for faculty members as assessors of
performance through direct observation
● Ensure CCCs adhere to pertinent institutional policies
● Share best practices from within the institution, nationally and
internationally
● Identify opportunities to enhance resources necessary to optimize CCC
functioning at an institutional level

7
ACGME
● Enhance progress toward competency-based education with outcomes
data
● Establish national benchmarks for the trajectory of resident/fellow skills
acquisition that can be used for each specialty
● Provide better measures for public accountability
● Enable continuous quality improvement of GME programs
● Document the effectiveness of the nation’s GME to prepare graduates to
meet the needs of the public
A program’s creation of a CCC is, in itself, a “developmental” process. Next, this
guidebook will briefly review of the current ACGME requirements for a CCC,
effective July 1, 2019. Programs may identify gaps and potential enhancements
through their CCCs by comparing what they have in place to meet the
requirements. For programs either beginning to institute a CCC, or looking to
enhance an existing CCC, the next few pages offer a practical roadmap.

8
Part 2: CCC Structure and Membership
Designing and Creating a CCC
To design, create, and operate a CCC, it is useful to start with the requirements.
The ACGME requirements for a CCC are found in the Program Requirements (both
in the Common Program Requirements for Residencies, Fellowships, One-Year
Fellowships, and Post-Doctoral Education Programs, and also in the specialty- and
subspecialty-specific Program Requirements). CCC requirements are generally the
same for all programs and are considered “core” requirements—or essential and
required for all GME programs. The CCC is mentioned in Program Requirement
III.A.4.b) for those specialties that allow exceptions to resident eligibility
requirements. CCCs are also mentioned in the Background and Intent related to
Program Requirement IV.A.3. regarding the Educational Program. Most of the
requirements and description of CCCs are found in Section V.A. of the Common
Program Requirements, which addresses Resident/Fellow/Post-Doctoral Education
Fellow Evaluation.
The ACGME International Foundational Program Requirements are similar. “The
program director must appoint the CCC [V.A.1.]; (It) should be composed of
members of the program faculty [V.A.2.a)]; have a written description of its
responsibilities, including its responsibility to the Sponsoring Institution and to the
program director [V.A.2.b)]; participate actively in reviewing all resident evaluations
by all evaluators [V.A.2.c).(1)]; and, making recommendations to the program
director for resident progress, including promotion, remediation, and dismissal.
[V.A.2.c).(2)]” [
www.acgme-
i.org/Portals/0/FoundInternational03312016.pdf?ver=2016-04-25-084913-527]
These are minimum requirements; once the program CCC fulfills the Common
Program Requirements, and any specialty-specific and board requirements, they
are free to innovate!
Step 1: Review Section V.A. of the relevant specialty-specific Program
Requirements.
While there are no specific requirements for the CCC in the Institutional
Requirements at present, there are at least two institutional requirements that
should be considered. The Sponsoring Institution is responsible for programs’
development of “promotion criteria” and criteria for renewal of a resident’s/fellow’s
appointment (Institutional Requirement IV.C.), and those conditions for
reappointment and promotion to a subsequent PGY level must be in the contract or
letter of appointment. (Institutional Requirement IV.B.2.d)).
Many CCCs may de
facto “act” as promotion committees and apply their judgement of resident/fellow
performance to recommend resident/fellow renewal and promotion to the next
program year. The Common Program Requirements specify that “at least
annually... a summative evaluation of each resident that includes their readiness to
progress to the next year of the program, if applicable” must be conducted.
[Common Program Requirement VI.A.1.e)] Although not stated explicitly, it is likely
that an effective CCC will have collaborated with the program director to identify the
promotion criteria, or at the very least, align Milestones performance with them. The
CCC should inform the program director of its review so that the program director

9
can truly exercise the responsibility, authority, and accountability for promotion of
residents. [Common Program Requirement II.A.4.]
It is important to recognize that the Milestones do not represent the totality of any
discipline, but rather form a foundational core. They are intended to be used as a
formative framework to guide curricula, assessment, and CCC deliberations in
programs. The Milestones will also ultimately guide and inform CCC deliberations
that lead to a summative judgment to allow the program director to decide upon an
individual resident’s/fellow’s readiness for entrustment decisions, promotion, and
graduation. However, the Milestones should not be used as the sole criteria for
these important decisions. Programs should read the companion Milestones
Guidebook that provides specific recommendations and guidance on how best to
use the Milestones in residency and fellowship programs
(http://www.acgme.org/Portals/0/MilestonesGuidebook.pdf
).
Programs should periodically review their policies, with input from the DIO and
institutional Legal and Human Resources team members, to address:
● Needed clarifications or adjustments in the criteria for promotion, program
completion, remediation, and/or non-renewal.
● Needed changes in the “agreement of appointment” necessary to reflect
Milestones reporting to the ACGME.
● Necessary changes in the grievance policy, ensuring program policies are
always aligned with the institutional policy.
Changes may not be necessary. However, the ongoing development of the CCC
provides an excellent opportunity to review current performance standards,
promotion/program completion criteria, and assessment processes, and align the
Milestones and the work of the CCC with them. The DIO, Office of GME, Legal,
and HR resources may provide useful guidance.
Step 2: Assess How Well You Know the CCC Requirements
Appendix B provides a multiple choice “quiz” on the current ACGME requirements
for a CCC; Appendix C includes a series of case studies.
Faculty development opportunities may include having the CCC members, the
members of the core faculty, and the program and/or institutional leadership take
the quiz, discuss the case studies, or use one or more readings as an
“educational” journal club. These resources may also be used with the program’s
residents/fellows to help them better understand the role of the CCC in the
program’s assessment process.
The ACGME’s CCC requirements are listed in Table 2. These are the same
across all programs, and the ACGME Review Committees are not able to further
specify requirements in these areas without approval from the ACGME Committee
on Requirements. There are minor differences in the wording but not the
underlying intent of the Common Program Requirements, for each type of GME
program: residency; fellowship; one-year fellowships; and post-doctoral education
programs. For example, requirement A.1.c).(2) in both the Common Program
Requirements for fellowship programs and for one-year fellowship programs, state
“that the program must provide [objective performance evaluation] to the CCC for

10
its synthesis of progressive fellow performance and improvement toward
unsupervised practice.”
Requirement A.1.c).(2) in the Common Program Requirements for post-doctoral
education programs state that, “the program must provide (objective performance
evaluation) to the CCC for its synthesis of progressive post-doctoral fellow
performance and improvement…”
Appendix D provides a template that may help programs design and/or evaluate
the CCC, by “walking through” its various components. Filling in the blanks can
generate a draft document that will provide a written description of the
responsibilities of the CCC.
The ACGME no longer requires a written description of the CCC. However,
programs may still benefit from a written description, which may serve as an
important communication tool for residents/fellows and faculty members. It may
also provide a concise description of the expected roles for faculty members on
the CCC, that they could use to support their own promotion, and/or to help the
program director negotiate for needed resources from the Division, Department, or
Institution.
Creating, developing, and improving a CCC to optimize its function does require
considerable time and effort. The long-term effectiveness of a CCC can be
facilitated by institutional support from the DIO for shared resources across
programs within an institution, and for appreciating that there will be a learning
curve for new programs. Ultimately, the CCC process will help programs do what
they have always been responsible for doing, but with greater structure, clearer
purpose, and more standardization across programs nationally.
Table 2 lists the CCC functions for a residency as described in the Common
Program Requirements (Residency), and for programs with ACGME Osteopathic
Recognition.
Table 2. Common Program Requirements for a CCC - Residency Version
(effective July 1, 2019)
Description of Requirements in Specialty/Subspecialty Programs
Common
Program
Requirement(s)
or Background
and Intent
section
(The program must) provide (objective performance evaluation based on
the Competencies and the specialty-specific Milestones, and must use
multiple evaluators, e.g., faculty members, peers, patients, self, and other
professional staff members) “to the CCC for its synthesis of
progressive resident performance and improvement toward
unsupervised practice.”
V.A.1.c).(1)-
V.A.1.c).(2)

11
The program director/designee with “input from the CCC” must meet
with/review with each resident/fellow the semi-annual performance
evaluation, including specialty-specific Milestones progress, assist in
developing individualized learning plans, and develop plans for those
failing to progress.
V.A.1.d)
The program director must provide a final evaluation for each resident
upon program completion; specialty -specific milestones, and when
applicable specialty-specific Case Logs must be used as tools to ensure
residents are able to engage in autonomous practice; the final evaluation
must “consider recommendations from the CCC.”
V.A.2.a).(2).(c).
The program director must appoint CCC members.
V.A.3.
There must be a minimum of three program faculty members, at least one
of whom is a core faculty member.
V.A.3.a)
Additional members must be faculty members from the same or other
programs, or other health professionals who have extensive contact and
experience with the program’s residents/fellows.
V.A.3.a).(1)
The CCC must review all resident/fellow evaluations at least semi-
annually.
V.A.3.b).(1)
The CCC must determine each resident/fellow’s progress on the specialty-
specific Milestones.
V.A.3..b).(2)
The CCC must meet prior to residents’/fellows’ semi-annual evaluations
and advise the program director regarding progress.
V.A.3.b).(3)
The (‘delineation of resident responsibilities in patient care, progressive
responsibility for patient management and graded supervision’) are
generally described by PGY level and specifically by Milestones progress
as delineated by CCCs.
Background and
Intent for IV.A.3
If the Review Committee allows program applicants to be accepted
through an “exception” process, these residents/fellows “must have an
evaluation of their performance by the CCC within 12 weeks of
matriculation.”
III.A.4.b)
FOR PROGRAMS WITH OSTEOPATHIC RECOGNITION
Osteopathic
Recognition
Requirements
The Director of Osteopathic Education or a designee should be a member
of the program’s CCC.
V.A.1.a)

12
The program’s CCC or a sub-committee of the CCC must review the
progress of all designated osteopathic residents in the program as it relates
to [osteopathic principles and practice] OPP.
V.A.1.b)
[The CCC or a subcommittee of the CCC must] include at least two
osteopathic faculty members, which may include the Director of
Osteopathic Education.
V.A.1.c).(1)
The CCC must review all designated osteopathic residents’ evaluations
semi-annually as these relate to the Osteopathic Recognition Milestones.
V.A.1.c).(2)
The CCC must prepare and ensure the reporting of Osteopathic
Recognition Milestones evaluations for each designated osteopathic
resident semi-annually to the ACGME.
V.A.1.c).(3)
The CCC must advise the program director and Director of Osteopathic
Education regarding resident progress, including promotion, remediation,
and dismissal from a designated osteopathic position.
V.A.1.c).(4)
General Principles for CCCs
The size of the residency or fellowship will affect how the program director
constructs the CCC process. For the purposes of this guidebook, “small programs”
have fewer than 15 total learners; “medium programs” have 15 to 75 learners; and
“large programs” have more than 75 learners.
One committee or more:
● Large programs may need to have several CCCs. There is a great deal of
variety in how programs construct sub-CCCs. Some programs create sub-
CCCs based on PGY, having separate sub-CCCs responsible for each PGY
cohort; others have a sub-CCC follow a cohort longitudinally from entering
residency through graduation; and still others have separate sub-CCCs for
large curricular themes or components within the program (e.g., a CCC that
will review resident/fellow scholarship, procedural competence/Case Logs,
or quality improvement activities). Others simply divide the residents into
more manageable numbers. Some CCCs have each member responsible
for a subset of the Competencies.
● If sub-CCCs are used, it is essential that they still have robust
membership and review processes to ensure all residents and fellows
are thoroughly reviewed, discussed, and provided with an opportunity
to receive high quality feedback. There also needs to be a mechanism
to integrate information from sub-CCCs and ensure each sub-CCC
has a shared mental model with the overall program and is using the
same standards and procedures.
● For medium-sized or small programs, a single CCC may be able to oversee
all residents/fellows. Program directors will use their discretion to determine
whether one CCC is sufficient based on the curricular design of the program
and local resources.
13
Committee membership:
● Appointment. The program director must appoint the CCC, which at a
minimum must include three faculty members, at least one of which is a
core faculty member in the program. Three is the smallest number of
individuals required for a truly good discussion. Some program directors will
want to use “term limits” and have a subset of CCC members rotate off each
year to refresh the CCC periodically and retain experience.
● Size. The literature suggests that a group size of five to seven individuals is
generally considered ideal, and no more than eight to 10 individuals in a
group is recommended for optimal committee functioning. CCC members
should regularly teach and observe residents/fellows.
● Diversity. The literature suggests that diverse groups make better decisions
than homogenous groups. To the extent possible, program directors should
try to balance CCCs in terms of academic rank, gender, race/ethnicity,
program role, and professional focus. (Hauer, 2016)
● Additional Members. The program director may appoint additional CCC
members from the same or other programs, or other health professionals
who have extensive contact and experience with the program’s residents
(e.g., nurses, physician assistants, nurse practitioners, social workers, etc.).
● Osteopathic Representation. If the program has Osteopathic Recognition
and has osteopathic-focused residents/fellows, there must be two
osteopathic-focused faculty members on the CCC, and the Director of
Osteopathic Education (or a designee) must also be on the committee.
● Chief Residents. Chief residents who have completed a core residency
program may serve on the CCC. Chiefs who are residents in the same
ACGME-accredited program (the chief title distinguishing their final year of
training) cannot serve on the CCC. It is important to make sure any chief
selected is comfortable with this role. A chief who completed the program
within the last year or two years may be too personally close to the
residents to be candid in this evaluation activity.
● Role of Advisors/Mentors. Program directors may want to consider whether
there is an inherent conflict of interest if a faculty member is an advocate for
a resident/fellow (as the resident’s advisor or mentor) and a “judge” of
performance (as a CCC member). On the other hand, advisors and mentors
may benefit from being observers to the CCC and contributing information
to the discussion and hearing the deliberation. This may better help them
convey the impressions of the CCC when they provide feedback to their
resident/fellow advisees.
Other considerations:
● The “right size” of a committee is large enough to reflect the diversity of
perspectives and small enough to be manageable. CCC members must be
able to attend meetings, actively participate, and engage in faculty
development about their CCC role.
● CCC members must be committed and able to attend all or nearly all
meetings; erratic attendance will not allow the continuity critical to assessing
resident/fellow performance over time. Each member must be willing to
make honest decisions, even when it is challenging.
● With regards to term limits and duration of service, consider whether
14
appointments should be “in perpetuity,” or for a defined time period. In
perpetuity appointments should be coupled with regular addition of new
members for fresh perspectives; if enacting term limits, consider staggering
appointments so that not everyone on the CCC turns over at once.
● Some programs have found value in having a “public member” to represent
a societal view, similar to the practices of many organizations’ boards,
including the ACGME’s. This is not an ACGME requirement, but anecdotally
some programs have described benefits of adding a non-faculty member,
such as a social worker, patient safety officer, or member of a
hospital/health system/school patient advisory board.
● Small programs may be challenged in identifying three CCC members if
they have a limited number of faculty members. Many fellowships will likely
be in this position. Three program faculty members, one of whom must be a
core faculty member (denoted as such on the program’s Faculty Roster),
are essential. In addition to program faculty members, consider inviting
faculty members from the core residency program, other related disciplines,
or settings in which the resident(s)/fellow(s) have substantial exposure
and/or provide substantial consultation. Many small programs are also tied
to specific clinical settings; consider inviting faculty members from such
settings who have ongoing contact with the resident(s)/fellow(s) to sit on the
CCC (e.g., a nurse leader from a dialysis unit for a nephrology fellowship, a
nurse anesthetist for a surgery fellowship, a patient safety officer, or a
discharge planner from a specific clinical unit).
● Medium-sized programs may also encounter some of the same challenges
in finding faculty CCC members as small programs.
CCC Chair:
Some boards or Review Committees may place restrictions on who can chair a
CCC. The American Board of Anesthesiology (2019), for example, does not allow
the program director to chair the CCC.
Other boards are silent on this issue.
Programs should reflect on who would be the right chair for the CCC: the program
director? the associate program director? another faculty member? a rotating
responsibility among members? voted on by CCC members? Program directors
should select the individual who will best solicit broad input regarding
resident/fellow performance and ensure all voices are heard.
CCC chairs should work with the CCC members to ensure a safe environment in
which all can freely share their judgements and concerns. The chair can mitigate
“hierarchy” within the group by having the most junior member(s) speak first. The
chair should ensure all residents are discussed, not just those perceived as having
problems or concerns. Table 3 identifies additional guidelines for the optimal CCC
chair.
Table 3: Guidelines for Committee Chairs, adapted from French et al. (2014)
Chairs should:
● Be the Milestones “expert” for the committee or designate another
committee member who will serve in this role.
● Encourage a confidential positive working environment and open
communication from all members.
● Ensure members know their roles, as well as the latest versions of the
Milestones and the CCC process.
15
● Engage members in developing a shared mental model for the
Milestones and the assessment tools.
● Use best practices in effective group processes; for instance, employ a
structured format to gain information from each committee member;
obtain input using the same order of members, get perspectives of the
most junior member first (See Part 4, Running the CCC Meeting).
● Keep meetings on task and move toward the common goal.
● Make certain the coordinator or designated member maintains
documentation and meeting minutes.
● Understand the typical assessment methods used by the program, as
well as their limitations.
● Develop a plan for the professional development of CCC members
(perhaps a dedicated period of time at the beginning or end of each
meeting, or an assigned article to read before the meeting).
● Anticipate biases on the part of both oneself and committee members,
and intentionally cultivate greater insight on biases and strategies to
mitigate them.
Program director role:
The Common Program Requirements do not proscribe a specific CCC role for the
program director. The program director can be a chair (except in anesthesia
programs), a CCC member, or an observer, or not attend CCC meetings at all. The
Background and Intent for this section of the Common Program Requirements
describes the rationale for this degree of flexibility. If present, the program director
should not detract from the participation of other team members by prematurely
inserting a personal perspective on a given resident’s/fellow’s performance. In the
same way, the program director should not determine the Milestones ratings of
each resident/fellow and then bring these to the CCC for ratification. The CCC
should be able to perform its assessment of resident/fellow competence freely,
judged against the Milestones, to convey to the program director.
Program directors who attend CCC meetings should defer to the chair, to make
sure other CCC members’ voices are encouraged (e.g., asking other members to
discuss residents/fellows and reach consensus decisions before adding their own
comments). Some program directors find it extremely useful to have another faculty
member chair the CCC, so they can function better as the resident/fellow advocate
and mentor and avoid the residents/fellows viewing the CCC’s judgments as “only”
those of the program director. On the other hand, the program director indeed has
the final responsibility for reporting and determining the Milestones ratings for each
resident/fellow and should also ensure the residents/fellows are aware of how their
performance on the Milestones has been reported to the ACGME.
Coordinator role:
Program coordinators are essential in the CCC process through their involvement
with many, if not all, aspects of the program, and their knowledge of the
residents/fellows. Program coordinators frequently distribute and collect results
from assessment tools. They may also participate in multisource feedback by using
assessment instruments to share valuable and often unique perceptions of an
individual resident’s/fellow’s abilities in interpersonal and communication skills,
teamwork, and professionalism.
16
Program coordinators may attend CCC meetings in an administrative role at the
discretion of the program director. They can assist in the collection, preparation,
organization, and distribution of assessment data; take minutes; and capture key
aspects of the discussion. They can observe group process using some of the tools
and frameworks provided below and provide feedback to the CCC as part of a
continuous quality improvement (CQI) process. Following a CCC meeting, the
program coordinator can facilitate the communication of results to the program
director (if not in attendance); schedule meetings with individual residents/fellows
and the program director or designated faculty member to review decisions,
including Milestones status; and electronically submit Milestones information on
each resident/fellow to the ACGME. The coordinator can also capture information in
the CCC “debriefs” that may lead to improvements in the CCC process at the next
meeting. However, the program coordinator cannot be a CCC member, or make
judgments in or after the meeting regarding resident/fellow performance.
Coordinators should provide assessment and feedback through the program’s
assessment system, such as by participating in multisource assessment
instruments.
Members of the CCC:
Each member of the CCC will have various tasks to complete prior to, during, and
after each meeting. Table 4 summarizes these.
Table 4: Role/responsibility of each CCC member, modified from French et al.
Guidelines for Committee Members:
● Understand the purpose and responsibilities of the CCC
● Know role on the committee
● Recognize sources of likely biases and take steps to mitigate their impact
● Work with other members to develop a shared mental model of the
Milestones
● Follow through with assigned tasks (such as pre-review and synthesis of
resident/fellow performance data)
● Participate in ongoing professional development (the Milestones, best
practices in assessment, effective group process, understanding and
identifying bias)
● Facilitate a collegial, respectful atmosphere within the committee
● Use best practices to support a robust group process
● Ensure own honest “voice” is heard along with those of colleagues
● Maintain confidentiality
● Help orient new members
● Contribute to ongoing improvement of the CCC processes
Meetings:
Logistics of meetings should include location, frequency, and length. CCCs may
wish to meet more frequently than the minimum requirement of twice yearly. There
is no one way to accomplish their task. A study of 116 emergency medicine
program directors found that slightly over half met quarterly, and a third monthly.
(Doty, 2016) Approximately 40 percent of the CCCs reviewed the entire program at
a single sitting, and a third reviewed an entire class of residents at a meeting, such
as all PGY-1s.

17
References
1. ACGME. ACGME Common Program Requirements (Fellowship).
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRFello
wship2019.pdf. 2020.
2. ACGME. ACGME Common Program Requirement (One-Year Fellowship)
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPROneY
earFellowship2019.pdf. 2020.
3. ACGME. Osteopathic Recognition Requirements.
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/801Osteo
pathicRecognition2018.pdf?ver=2018-02-20-154513-650. 2020.
4. ACGME. ACGME Common Program Requirements (Post-Doctoral Education
Program).
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRPost-
Doctoral2018.pdf. 2020.
5. ACGME. ACGME Common Program Requirements (Residency).
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResid
ency2019.pdf. 2020.
6. ACGME International. ACGME International Foundational Program
Requirements for Graduate Medical Education.
https://www.acgme-
i.org/Portals/0/FoundInternational03312016.pdf?ver=2016-04-25-084913-
527. 2020.
7. ACGME. ACGME Institutional Requirements.
https://www.acgme.org/Portals/0/PFAssets/InstitutionalRequirements/000Insti
tutionalRequirements2018.pdf?ver=2018-02-19-132236-600. 2020.
8. American Board of Anesthesiology. 2019 Policy Book. Page 14.
http://www.theaba.org/PDFs/BOI/2019-Policy-Book
. 2020.
9. Doty CI, Roppolo LP, Asher S, et al. How do emergency residency programs
structure their Clinical Competency Committees? A survey. Acad Emerg Med.
2015;22(11):1351-1354.
https://onlinelibrary.wiley.com/doi/full/10.1111/acem.12804
. 2020.
10. French JC, Dannefer EF, Colbert CY. A systematic approach toward building
a fully operational Clinical Competency Committee. J Surg Educ.
2014;71(6):e22-e27.
https://www.sciencedirect.com/science/article/abs/pii/S193172041400107X?v
ia%3Dihub. 2020.
11. Hauer KE, Cate OT, Boscardin CK, et al. Ensuring resident competence: A
narrative review of the literature on group decision making to inform the work
of Clinical Competency Committees. J Grad Med Educ. 2016;8(2):156-164.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4857505/
. 2020.
18
Part 3: Preparing for CCC Meetings
Developing a Shared Mental Model
Perhaps the most important aspect of preparing for a CCC meeting is to make sure
the members develop a shared mental model of what resident/fellow performance
looks like, and understand their roles and responsibilities on the committee, as well
as how the CCC operates to judge resident/fellow performance. Developing a
shared mental model of the Competencies and the Milestones is essential. This will
usually necessitate a “meeting before the meeting,” or allocating sufficient time at
the beginning of a CCC meeting for this discussion before a new CCC gets started
on its first reviews. CCCs should also engage in ongoing dialogue to enrich and
deepen their understanding and mental model over time. Having a written
description of the CCC process (though no longer required by the ACGME) and
providing faculty development for committee members, can facilitate this. Some
programs find it useful to discuss a relevant article at a CCC meeting as part of
faculty development. See the references and annotated bibliography for some
suggestions.
Faculty members should reach a common understanding on the meaning of the
narratives of each milestone in the context of the specialty. This will almost always
require group conversation. It may be worthwhile to have each faculty member
perform self-assessment, using the specialty-specific Milestones, as a faculty
development exercise. Faculty members should be trained to compare each
resident’s/fellow’s performance to the Milestones as a whole, not just to the
performance of other or ‘typical’ residents/fellows in the program.
Note that as Milestones 2.0 is available for individual specialties, a Supplemental
Guide is also available. The Supplemental Guide includes the intent of the
subcompetency along with examples for each level, assessment methods, and
resources. The Supplemental Guide can be used to develop a shared mental
model and determine examples for each program. The CCC can individualize the
Supplemental Guide and use it as it considers resident development over time.
Members may also benefit from individually assessing recent program graduates
using the new Milestones, and then discussing as a committee to determine a
group consensus as another potential faculty development exercise.
Inventory Where Milestones are Represented in the Program
Competency-based medical education entails defining outcomes of education and
training, which then guide development of milestones to chart progress through the
course of a residency and fellowship program. Each program must determine which
of its assessment tools and activities address each milestone. CCCs should
inventory (or review an inventory conducted by others) where each milestone is
currently taught and assessed in the program to create a map that guides design
of curricular experiences. Teaching may occur on a specific rotation, or in the
context of a program activity, such as “leading morbidity and mortality rounds.”
Appendix E lists assessment methods for each of the Competency domains with
some representative examples.
19
The inventory should help to identify gaps in both curriculum and assessment. The
CCC can identify how to best address these gaps, perhaps by delegating the
review to a designated faculty member.
Shift from Assessment of Learning to Assessment for Learning
The foundation of competency-based education requires robust assessment with
regular honest feedback to each learner. This requires a large amount of data. The
CCC is in the perfect position to analyze how assessments drive learning, inform
the judgement of resident progress, and improve the overall quality of the program.
The assessment information and data that inform CCC deliberations necessitate a
comprehensive and intentional overall program assessment strategy. It should
follow several key principles:
● The Milestones were never meant to be used as a standalone assessment tool,
especially for short rotations (e.g., two to 12 weeks). Some programs continue
to use the entire Milestones Set for end-of-rotation evaluations. This typically
works poorly despite the fact this may seem a logical expedient, and even
helpful to faculty members, to better acquaint them with the Milestones and the
skills, attitudes, and behaviors they need to assess. However, there are several
major issues. First is the concept of cognitive load – the more you ask faculty
members to judge in shorter periods of time, the more difficult it is to truly
assess all the Competencies. Faculty members may feel pressed to assess
residents on milestones they did not directly observe, leading to range
restriction (i.e., using a very limited range of the Milestone levels), “straight
lining” (i.e., residents rated exactly the same on all Milestones), and halo
effects (i.e., strength in one area, such as Medical Knowledge, “spills over” into
ratings of other areas, especially if they were poorly assessed).
● Programs may consider a “retreat” to take each milestone and map out where it
is taught and assessed, as well as how it is assessed in the program. This will
highlight any gaps and opportunities for improvement. Frequently this can be
done collaboratively, either with other programs in the same state or region in
the same specialty, or with other programs of different specialties within the
same institution.
● The assessment program will need to include multiple forms of assessment
with multiple sampling using multiple assessors. No single assessment method
or tool is sufficient to judge something as varied and complex as clinical
competence. While end-of-rotation evaluations have some value, an
overreliance on global, end-of-rotation evaluations should be avoided.
● The combination of assessments will depend to some extent on the specific
needs of the specialty and the local context. Consult the Milestones Guidebook
for more information.
● At a minimum, core methods of assessments should include direct observation
of a specific component (e.g., care of individual patients, procedures, hand-
offs), multi-source feedback, multiple choice test/in-service examination,
longitudinal evaluations (e.g., rotational evaluation forms), audit of clinical
performance, and simulation where appropriate. The specific assessment tools
used will depend on the specialty and local context. The key point to remember
is that the true assessment “instrument” is not the tool or form itself, but rather
the individuals using it. The tool or form simply guides the individual performing
20
the assessment. CCCs should be cautious not to place an overreliance on
global, end-of-rotation evaluations, which too often fail to provide meaningful
comments and are limited by their scales and items.
● Faculty members and others involved in assessing residents/fellows will need
training in the use of and interpretation of data from the selected assessment
tools.
Some opportunities for assessments include the methods included in Appendices E
and F. Please note the lists are not comprehensive; consult the Milestones
Guidebook and the recent overview by Lockyer et al. (2017).
Preparing for Specific CCC Meetings
Another key pre-meeting activity is preparing the assessment data for review. It is
important to plan how all assessment information, including information that occurs
at the meeting, and from information gained through hallway conversations or other
informal sources, will be collected and summarized. Many resident management
systems (RMS) have tools available to aggregate evaluations, such as spider
graphs (aka radar plots), visual plots, and dashboards. These have been shown
both to make CCC discussions more efficient and to help in giving feedback to the
residents following the CCC meeting. Some learning management systems have
the ability to perform basic statistics on assessment data and may display visually
with dashboard tools such as spider graphs. While this is helpful, a word of caution:
simple means (i.e., averages) of aggregated assessments can be misleading,
especially if ranges and confidence intervals are not provided. In these cases, an
important outlier assessment might be missed and not properly reviewed and
discussed. Also remember the cardinal GIGO (“garbage in, garbage out”) rule: if the
quality of the assessments being used to produce aggregate data, such as
averages, is poor, then not even fancy statistics can make the assessment
information better.
It is also important for CCCs to examine the assessment data longitudinally. This
can be especially helpful once residents and fellows have acquired several cycles
of Milestones judgments, typically starting in their second year. The 2019
Milestones National Report includes predictive probability value (PPV) tables for
most GME programs that can assist CCCs in identifying residents with suboptimal
developmental trajectories within a subcompetency.
Larger CCCs may assign members a subset of the residents/fellows for whom to
review the assessment information in advance and prepare a preliminary review.
An individual member may be responsible for reviewing all measures of the
assigned residents’/fellows’ performance and preparing a synopsis that is brought
to the meeting and discussed with the full CCC. Some programs have individual
members complete Milestones assessments on each resident or fellow and have
the coordinator aggregate the information in advance of the meeting.
Suggested practices:
1. Synthesize performance information (done by the coordinator or assigned
CCC member) in advance of meeting.

21
2. Share written performance information about individual resident/fellow
performance during the CCC meeting (e.g., in a handout, a projection in the
room).
3. Train CCC members on how to interpret aggregated, synthesized performance
information about individual residents/fellows. This means that CCC members
must understand the nature and quality of the synthesized assessment data.
4. Maintain the confidentiality of the information. Failure to do so will undermine
trust in the Milestones and the CCC process.
5. Increase the use of direct observation, video logs, outcomes from actual
clinical performance, patient experience, and team member data as data
sources.
6. Practice good group process.
7. Review the specialty’s PPV tables in the 2019 Milestones National Report
.
8. Identify what’s not being assessed that may be critical to authentically judge
Milestone performance. CCCs have been shown to neglect resident/fellow
quality improvement, patient surveys, and actual clinical performance data.
Prior to the implementation of the Milestones, Hauer’s 2015 study of 34 program
directors at five institutions discovered that most CCCs relied on global, end-of-
rotation evaluations rather than using programmatic assessment with multiple tools
and data points, focused on problem residents more than they spent time
discussing the typical residents, and lacked faculty development or training of CCC
members. A small, single-institution study found that faculty members’ evaluations
received substantial weight in CCC deliberations in a large internal medicine
residency that used sub-CCCs, but the sub-CCCs weighed comments next in
importance. (Epkenyong, 2017) A study of 14 pediatric CCCs found that only two
considered participation in quality improvement projects (Schumacher, 2018).
Finally, a study by Watson, et al. (2017) found patient surveys identifying 13 of 19
factors the CCC used as important to evaluation; performance data was not
included in the 19 factors. Each of these studies speaks to the need to collect
robust data and provide deliberate, ongoing faculty development for those who
serve on the CCC, especially in the Milestones era.
Dashboards
A strategy for efficient data synthesis and display facilitates the work of the CCC.
Data synthesis remains challenging for many programs that may share too much,
too little, or poorly organized data with CCC members. A dashboard offers a
platform for high-level data display, combined with drill-down options for more detail
on quantitative and qualitative measures of learner performance. This information,
combined with display of metrics indicating expected levels of performance,
enables evidence-informed feedback discussions between residents/fellows and
their faculty advisors or coaches to inform robust learning planning.
Some programs document their CCC deliberations through their resident
management system (RMS). The RMS can create a Milestones evaluation
composite, and often graphical plots, which can be shared electronically with a
resident/fellow and stored with all the other resident/fellow evaluations. (Friedman,
2016; Johna, 2015)

22
Key Point: Whatever method is used to “pre-digest” and organize the data for
review, programs should ensure processes and/or standard protocols are in place
to ensure a systematic, consistent approach to the pre-review and the meeting
preparation process. Programs should not simply use statistical means (i.e.,
averages) or a single type of data to make CCC determinations. Narrative data
collected from assessment tools represents important additional information for the
CCC. As noted above, the Milestones do not represent the totality of the discipline,
and informed human judgment is still a critical component of the CCC process.
Much important and useful assessment information is attained through effective
group discussion at the CCC meeting.
References
1. Ekpenyong A, Baker E, Harris I, et al. How do clinical competency committees
use different sources of data to assess residents' performance on the internal
medicine milestones? A mixed methods pilot study. Med Teach.
2017;39(10):1074-1083.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1353070?journal
Code=imte20. 2020.
2. Friedman KA, Raimo J, Spielmann K, Chaudhry S. Resident dashboards:
helping your Clinical Competency Committee visualize trainees' key
performance indicators. Med Educ Online. 2016;21:29838.
https://www.tandfonline.com/doi/full/10.3402/meo.v21.29838
. 2020.
3. Hauer KE, Chesluk B, Iobst W, et al. Reviewing residents' competence: a
qualitative study of the role of Clinical Competency Committees in performance
assessment. Acad Med. 2015;90(8):1084-1092.
https://journals.lww.com/academicmedicine/fulltext/2015/08000/Reviewing_Resi
dents__Competence__A_Qualitative.25.aspx. 2020.
4. Johna S, Woodward B. Navigating the Next Accreditation System: A dashboard
for the Milestones. Perm J. 2015;19(4):61-63.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4625996/
. 2020.
5. Lockyer J, Carraccio C, Chan MK, et al. Core principles of assessment in
competency-based medical education. Med Teach. 2017;39(6):609-616.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1315082?journal
Code=imte20. 2020.
6. Schumacher DJ, Michelson C, Poynter S, et al. Thresholds and interpretations:
How Clinical Competency Committees identify pediatric residents with
performance concerns. Med Teach. 2018;40(1):70-79.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1394576?journal
Code=imte20. 2020.
7. Watson RS, Borgert AJ, O Heron CT, et al. A multicenter prospective
comparison of the Accreditation Council for Graduate Medical Education
Milestones: Clinical Competency Committee vs. resident self-assessment. J
Surg Educ. 2017;74(6):e8-e14.
https://www.sciencedirect.com/science/article/abs/pii/S1931720417302490?via
%3Dihub. 2020.
23
Part 4: Running the CCC Meeting, Including Effective Group Process
The CCC meeting can serve multiple purposes and the chair should ensure that all
members have a shared understanding about the role of the CCC and its goals. In
addition to rating residents’/fellows’ performance on the Milestones, other important
tasks can be accomplished, such as faculty development for the members, and
monitoring the quality of the assessment system. This section focuses on the many
processes and procedures that occur during CCC meetings. CCCs are charged
with rendering judgements about resident/fellow progress on the Milestones. It is
important to consider the following tips to bring the committee closer to realizing
this goal.
1) At the beginning of (or prior to) the meeting:
a. The CCC must have a shared understanding of its role in the assessment
system. Hauer et al. found that program directors had two different
perceptions of the role of the CCC: that of “problem identification” (i.e.,
focused on identifying the struggling residents/fellows) and “developmental”
(i.e., focused on helping all residents/fellows on their trajectory towards
achieving the Milestones). (2016) Although CCC chairs should contemplate
this prior to the meeting, during the meeting they should take opportunities
to move the group toward a developmental approach to benefit all learners
in the program.
b. Members should avoid coming to the meeting with a decision already
predetermined. It is inappropriate to use the CCC to simply confirm a
“verdict” about a resident or fellow from one member’s opinion or a set of
data. This may seem tempting; however, it significantly undermines the
benefit of having a group discussion, and pre-determined verdicts can be
inaccurate.
c. Plan for the group to discuss and agree on some ground rules or
“touchstones” for how the group will work together. Touchstones are simply
principles of engagement the group agrees to observe and to which
members hold each other accountable. For example, one touchstone might
be “all member opinions will be considered respectfully.”
2) During the meeting:
a. There should be a consistent and structured process for presenting each
resident/fellow during the meeting to ensure all members have an
opportunity to voice their opinions and any information that any given
member has about an individual resident/fellow is shared by the group.
CCC chairs should develop a structure or format to use during discussion
of each resident/fellow to ensure that key elements are not missed and so
that any relevant information that CCC members may have about a
resident/fellow that is not captured in the formal assessments can be
introduced. Some CCCs choose to assign residents/fellows to specific
members and ask the latter to present a summary about each of their
residents’/fellows’ performance. Donato and colleagues’ description of their
internal medicine residency CCC is one in which the resident is presented
in a “debate-like” format. (2016) Mentors present their resident(s) to the
CCC describing their accomplishments, and a second reviewer presents
challenges. The committee then discusses the presented information and
the mentor provides feedback to the resident.
24
b. Discussions of each resident/fellow may be enhanced by using charts,
pictures, spreadsheets, or other visual aids during the meeting. As noted
earlier, the PPV tables from the Milestones National Report can also help
guide the discussion. See Appendix G for an example of a PPV table.
c. At all times the chair should use guidelines for effective group process. It is
important to be mindful of issues of hierarchy that can negatively affect the
group dynamic. This is particularly an issue when a more senior faculty
member serves as CCC chair. One clear measure of the effectiveness of
the CCC is the willingness of all members to speak up. Consider using the
following techniques to minimize the effects of hierarchy:
i. Always start with the most “junior” person or the person most at risk in
the hierarchical chain.
ii. Chairs should, as a general rule, state their opinion last. In addition,
program directors, if present, should avoid stating their opinion early
on, if at all, depending on their role with the CCC. If present, the
program director’s role may be best as an observer, to “listen” to the
conversation and provide clarifying information if necessary, but not to
voice opinions, at least not until later in the discussion.
d. Effective group process is critical to the success of a CCC. The underlying
premise is that under the right circumstances, groups make better
decisions than individuals. The following are some examples of this
phenomenon, both within medical education and beyond:
i. Schwind et al. – deficiencies in surgical residents were uncovered via
group discussion, not during individual faculty member review. (2004)
ii. Hemmer et al. – professional lapses in medical students were only
identified as a result of formal group discussion. (2000)
iii. Thomas et al. – group discussions prior to the completion of the
evaluations of internal medicine residents in continuity clinic resulted
in higher reliability. (2011)
iv. The Wisdom of Crowds – author James Surowiecki, New Yorker
columnist, uses examples from a range of fields to demonstrate that
under the right circumstances (e.g., having diverse opinions, avoiding
groupthink) groups make better decisions than individuals. (2005)
e. CCC chairs and program directors need to be aware of the importance of
having a diversity of opinions expressed to enrich the group decision-
making process. The perspective each member brings to the discussions
(based on clinical expertise, research, medical education expertise, etc.)
is important. Research shows that minority opinions, even when “wrong,”
can lead to better decisions. In addition, CCC chairs need to have an
understanding of the factors that enable groups to function effectively
and
the potential biases that CCCs can encounter.
f. CCCs should have a shared mental model as to which assessment data
they need for their decision-making process. CCC chairs should take note
when this is not the case and should continue to work on building or
refining their “Milestones map” (see section on “Other uses of the CCC”).
In addition, committee members will likely bring information about many
residents and fellows not captured on completed assessment tools and
forms. The CCC provides a forum to hear this previously unshared
information. This information is critical to making a robust overall
assessment of each resident’s or fellow’s progress. However, if a program
finds that most of the useful information comes from CCC discussion and
25
is not written down on any assessment forms, it should consider revising
its assessment tools or processes and/or faculty development to solicit
better written/recorded information. Members may also need to spend
time discussing the “value” of different types of assessment data. They
may struggle with how much to value their own first-hand knowledge of a
resident’s or fellow’s performance versus information provided by
colleagues on formal assessments.
g. CCCs should have a shared understanding of how decisions will be made,
including how to deal with inadequate assessment data or lack of data. A
few studies have attempted to outline how CCCs make decisions.
Through observations of CCC meetings, Pack and colleagues describe
the process of making sense of assessment data that are difficult to
understand, and how the discussion of how to use the data enriches the
decision-making process. (Pack, 2019) Chahine and colleagues
performed a review of the literature on group process, and developed a
theoretical framework consisting of three “orientations” or approaches to
decision making by CCCs, namely “schema” (use of rules, guidelines),
“constructivist” (members work together to develop meaning and
understanding), and “social influence.” (2017) Also at play in this
framework are “moderators,” such as time, leadership style, etc., which
have an impact on the process.
h. Strategies to organize the conversation flow to ensure a systematic
approach with minimal bias can be inferred from the literature on clinical
reasoning. For example, Lambe (2016) and Croskerry (2003) found that
using cognitive forcing strategies allows for structured approaches to what
is discussed and how. Another recommendation from a review on
strategies to optimize clinical reasoning decision making is guided
reflection, in which decision making is slowed to avoid quick assumptions
and to lead individuals to consider information more deliberately. (Lambe)
The framing effect describes how individuals are swayed by whether a
scenario or option is portrayed positively or negatively. Bringing
awareness to the risk of the framing effect and overconfidence influencing
decisions is important for CCCs. (Saposnik, 2016)
i. How the decisions are made by the group is also important. The best
approach is for CCC members to choose the best description of the
residents’ or fellows’ abilities using the Milestones narratives, not the
numeric levels. Some studies have suggested that rating based on
narrative tends to be more discriminating. Too often when individuals start
by choosing a number rating, they will be more likely to try and justify that
rating. Encourage all members to focus on the narrative Milestones
descriptors.
j. The chair can determine the frame of reference that the CCC members
are using when rating the residents/fellows. The Milestones framework is
criterion-based, referring to specific expectations for all residents/fellows
to meet. However, sometimes faculty members may find themselves
comparing a given resident’s/fellow’s performance to themselves (self) or
to other residents/fellows (peer). If a resident/fellow has not rotated
through an experience over the past six months, and that hinders the CCC
in making a determination on one of the milestones, the CCC should
maintain the Milestone judgment from the previous reporting period.
26
k. The committee members will need to determine how best to spend their
time, e.g., time spent on struggling learners can often consume the
majority of the meeting, leaving little opportunity for discussing how to
assist residents/fellows with satisfactory or an even higher performance
level to create stretch goals. Large programs may address this in several
ways. To avoid having to discuss too many residents/fellows in one
meeting, some programs develop “subcommittees,” e.g., one for each
post-graduate year. These subcommittees may meet prior to the large
CCC meeting to discuss their assigned residents/fellows. In these
instances, subcommittees review each resident’s/fellow’s data and
discuss this in their meetings. During this process, they identify concerns
to bring to the full CCC. Other CCCs set up more than one meeting per
six-month cycle, e.g., once per month or every other month. They may
intentionally devote some of their meetings to be “formative” (i.e., focused
on ensuring they have all the necessary data and discussing performance,
but not assigning Milestones ratings), while other meetings are
“summative,” during which the committee actually rates the
residents/fellows on the Milestones. All residents/fellows, from the lower
performing residents and fellows to the “superstars,” need individualized
educational learning plans. Competence is the “floor,” and not the “ceiling”
of performance, and higher performing residents/fellows can be
challenged to develop further. Longer discussions tend to produce better
decisions and will likely produce better feedback.
l. Time pressure or trying to cover too many residents/fellows in one
meeting can produce lower quality decisions.
m. There should be a clear process for allowing the CCC to forward their
concerns about a given resident’s/fellow’s performance, their suggestions
for remediation, and their expectations for follow-up to either another
committee or the program director. There should also be clarity about the
expected outcomes of the meeting, which include not only the Milestones
ratings generated twice per year, but also feedback from the CCC to the
residents/fellows. The group will need to come to a consensus about the
type of feedback generated and develop a process for delivering it. The
CCC may also provide feedback to other stakeholders, such as the
program and core faculty members.
n. CCC chairs may choose to include some time during the meeting for
faculty development, such as regarding developing shared mental models
(as above), rater training, the pros and cons of various assessment
methods, building a “Milestones map,” etc.
3) Post-meeting:
a. The discussion about each resident/fellow should be captured and
documented (see Part 6: Legal Issues and Considerations). The
discussion and judgments of the CCC are legitimate and important
assessment information and should become part of each
resident’s/fellow’s record. This information should also serve as the
template for the feedback session with each resident/fellow. See section 5
for details regarding providing feedback to residents/fellows.
b. Transparency is an important principle in the ACGME’s accreditation
model. Accurately documenting and sharing the key components and
judgments with residents and fellows is a critical aspect of this principle.
27
c. Taking time at the end of each meeting to debrief how the meeting went
can improve processes at future meetings. The chair can generate a
discussion among the group by simply asking what went well, what could
be improved, and how members would like to see things move forward.
The coordinator, serving as an observer, can also provide useful feedback
for the whole group if appropriately guided and empowered to do so.
Thus, assess if the CCC is meeting its goals and determine how to
improve the next meeting.
d. In conjunction with assessment of residents/fellows, CCCs will
increasingly assess the performance of program. In assessing
resident/fellow performance against the Milestones, it will become clear
what is missing from the program’s assessment “toolkit,” and if there are
curricular gaps and redundancies. CCC deliberations can generate
behaviorally-specific feedback that will be useful to learners. But CCCs
will also identify feedback useful for faculty members. Some faculty
members will be recognized as role models for the timeliness, quality, and
quantity of their evaluations. The CCC can help these individuals to be
recognized, perhaps as part of promotion and tenure considerations, or
through incentives. Others may be tapped to coach fellow faculty
members whose evaluations could be improved.
e. The CCC should provide a synopsis of its findings to the Program
Evaluation Committee for its use in improving the assessment system
within the program.
f. The CCC, therefore, has an important role in the continuous educational
quality improvement of faculty members and the program, in addition to its
role in assessing residents/fellows.
It is recommended that the CCC revisit its purpose, shared mental model, and
procedures annually. Ongoing faculty development for CCC members to help
prevent the development of groupthink or drifting from the original aims and
procedures is critical.
As listed above, there are many factors to consider when planning or conducting a
CCC meeting. Should CCCs choose to maintain a written “policies and procedures”
document, it should be updated at least annually. CCCs should include the above-
mentioned processes in this document. Doing so not only fosters a quality
improvement approach to the workings of this committee but allow for greater
transparency of the CCC’s work to stakeholders.
Anticipating, Recognizing, and Mitigating Bias
Ensuring a fair and equitable assessment system constitutes a fundamental
obligation of the CCC to ensure that learners are afforded maximal opportunities to
learn and thrive in the program.
Especially as the diversity of learners continues to increase, CCC members require
awareness and training regarding bias in evaluations of learner performance.
Multiple studies and experts describe concerns about the risks of bias influencing
the evaluations of learners from students to postgraduate residents/fellows based
on gender and race/ethnicity. Emerging studies suggest that bias affects both
numerical and qualitative evaluations of learner performance. Quantitative ratings
28
of student and resident/fellow performance have been shown to be systematically
lower for women than men, (Dayal, 2017; Klein, 2019) and lower for
residents/fellows from backgrounds underrepresented in medicine. (Teherani,2018;
Backhus, 2019; Boatright, 2017) Narrative resident/fellow performance data also
reinforces stereotypes through use of different words to describe the performance
of different groups based on gender or race/ethnicity. (Rojek, 2019; Mueller, 2017;
Gerull, 2019; Salles, 2019; Ross, 2016; Isaac, 2011)
To address this important risk of bias influencing resident/fellow performance
ratings during CCC discussions, programs should do the following:
• CCC membership should include diverse members in terms of gender and
race/ethnicity. Diverse groups outperform homogeneous groups in terms
of the quality of their work and decision making. (Hong, 2004)
• All CCC members should participate in training on diversity, equity,
inclusion, and bias. Training can entail deepening one’s understanding of
unconscious bias and racism that permeates health care and medical
education. CCC members should appreciate how bias based on learners’
race/ethnicity or gender can impact both quantitative and qualitative
ratings of learner performance. Learners who are not white or who are
women receive lower numerical ratings and are less likely to be selected
for the Alpha Omega Alpha Honor Medical Society. (Boatright, 2017;
Mueller, 2017; Teherani, 2018) Women also receive less favorable ratings
on some milestones than men in some specialties (Dayal, 2017; Klein,
2019; Santen, 2019). Another study from Hamstra (2019) showed that in
pediatrics and some family medicine milestones, women scored higher.
Review of narrative comments about learner performance shows how
certain words may be systematically used more to describe individuals
based on the groups to which they belong. (Mueller, 2017; Rojek, 2019)
Through ongoing discussion and reflection, CCC members can share and
address their own perspectives and biases in order to recognize and
mitigate unconscious biases. (Morgan, 2018)
• The CCC should examine the program’s own data for any systematic
group differences in performance that signal bias in the evaluation data. In
their roles using CCC data to continuously improve the program, CCC
members should be vigilant for signs indicating how issues of race and
racism may be influencing residents’ learning experiences. (Karani, 2017)
• The CCC should discuss and reflect upon their performance ratings to
identify any areas in which bias may be influencing ratings and discuss
improvements to their processes. This reflection process can be
structured by reviewing the CCC’s data, including ratings for learners
based on gender and race/ethnicity. This review can uncover systematic
differences, as have been observed in some Milestones ratings showing
higher assessment of men than women in certain milestones traditionally
thought of as more ‘male’ characteristics. (Santen, 2019; Dayal, 2017)

29
References:
1. Backhus LM, Lui NS, Cooke DT, Bush EL, Enumah Z, Higgins R.
Unconscious bias: Addressing the hidden impact on surgical education.
Thorac Surg Clin. 2019;29(3):259-267.
https://www.thoracic.theclinics.com/article/S1547-4127(19)30015-5/fulltext
.
2020.
2. Boatright D, Ross D, O'Connor P, Moore E, Nunez-Smith M. Racial
disparities in medical student members in the Alpha Omega Alpha Honor
Society. JAMA Intern Med. 2017;177(5):659-665.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2607210
.
2020.
3. Chahine S, Cristancho S, Padgett J, Lingard L. How do small groups make
decisions? A theoretical framework to inform the implementation and study
of Clinical Competency Committees. Perspect Med Educ. 2017;6(3):192-
198. https://link.springer.com/article/10.1007%2Fs40037-017-0357-x
. 2020.
4. Croskerry P. Cognitive forcing strategies in clinical decision making. Ann
Emerg Med. 2003;41(1):110-20.
https://linkinghub.elsevier.com/retrieve/pii/S0196064402849459
. 2020.
5. Dayal A, O’Connor DM, Qadri U, Arora VM. Comparison of male vs. female
resident Milestone evaluations by faculty during emergency medicine
residency training. JAMA Intern Med. 2017;177(5):651-657.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2607209
.
2020.
6. Donato AA, Alweis R, Wenderoth S. Design of a Clinical Competency
Committee to maximize formative feedback. J Community Hosp Intern Med
Perspect. 2016;6(6):33533.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5161790/
. 2020.
7. Friedman KA, Raimo J, Spielman K, Chaudry S. Resident dashboards:
helping your Clinical Competency Committee visualize trainees’ key
performance indicators. Med Educ Online. 2016;21:29838.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4818357/. 2020.
8. Ekpenyong A, Baker EA, Harris I, et al. How do Clinical Competency
Committees use different sources of data to assess resident performance
on the internal medicine milestones? A mixed methods pilot study. Medical
Teacher. 2017;39(10):1074-1083.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1353070?jour
nalCode=imte20. 2020.
9. Gerull KM, Loe M, Seiler K, McAllister J, Salles A. Assessing gender bias in
qualitative evaluations of surgical residents. Am J Surg. 2019;217(2):306-
313. https://linkinghub.elsevier.com/retrieve/pii/S0002-9610(18)30631-7
.
2020.
10. Hauer KE, Chesluk B, Iobst W, et al. Reviewing residents’ competence: a
qualitative study of the role of Clinical Competency Committees in
performance assessment. Acad Med. 2015;90(8):1084-1092.
https://journals.lww.com/academicmedicine/fulltext/2015/08000/Reviewing_
Residents__Competence__A_Qualitative.25.aspx. 2020.
11. Hemmer PA, Hawkins R, Jackson JL, Pangaro LN. Assessing how well
three evaluation methods detect deficiencies in medical students’
professionalism in two settings of an internal medicine clerkship. Acad Med.
2000;75(2):167-173.

30
https://journals.lww.com/academicmedicine/Fulltext/2000/02000/Assessing_
How_Well_Three_Evaluation_Methods_Detect.16.aspx. 2020.
12. Hong L, Page SE. Groups of diverse problem solvers can outperform
groups of high-ability problem solvers. PNAS. 2004;101(46):16385-16389.
https://www.pnas.org/content/101/46/16385.long
. 2020.
13. Isaac C, Chertoff J, Lee B, Carnes M. Do students’ and authors’ genders
affect evaluations? A linguistic analysis of medical student performance
evaluations. Acad Med. 2011;86(1):59–66.
https://journals.lww.com/academicmedicine/Fulltext/2011/01000/Do_Studen
ts__and_Authors__Genders_Affect.22.aspx. 2020.
14. Karani R, Varpio L, May W, et al. Commentary: Racism and bias in health
professions education: How educators, faculty developers, and researchers
can make a difference. Acad Med. 2017;92(11S Association of American
Medical Colleges Learn Serve Lead: Proceedings of the 56th Annual
Research in Medical Education Sessions):S1-S6.
https://journals.lww.com/academicmedicine/fulltext/2017/11001/Commentar
y__Racism_and_Bias_in_Health_Professions.2.aspx. 2020.
15. Klein R, Julian A, Snyder ED, et al. Gender bias in resident assessment in
graduate medical education: Review of the literature. J Gen Intern Med.
2019;34(5):712-719.
https://link.springer.com/article/10.1007%2Fs11606-
019-04884-0. 2020.
16. Lambe KA, O'Reilly G, Kelly BD, Curristan S. Dual-process cognitive
interventions to enhance diagnostic reasoning: a systematic review. BMJ
Qual Saf. 2016;25(10):808-20.
https://qualitysafety.bmj.com/content/25/10/808.long
. 2020.
17. Morgan AU, Chaiyachati KH, Weissman GE, Liao JM. Eliminating gender-
based bias in academic medicine: More than naming the "Elephant in the
Room". J Gen Intern Med. 2018;33(6):966-968.
https://link.springer.com/article/10.1007%2Fs11606-018-4411-0
. 2020.
18. Mueller AS, Jenkins TM, Osborne M, et al. Gender differences in attending
physicians' feedback to residents: A qualitative analysis. J Grad Med Educ.
2017;9(5):577-585.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5646913/
. 2020.
19. Hamstra, SJ, Yamazaki, K, Holmboe, E. Gender group differences in
Milestone ratings: Exploring differences in ratings by individuals and Clinical
Competency Committees. Journal of Graduate Medical Education.
2019;11(6):722-731.
https://www.jgme.org/doi/full/10.4300/JGME-D-19-
00734.1?mobileUi=0. 2020.
20. Pack R, Lingard L, Watling C, Chahine S, Cristancho S. Some assembly
required: tracing the interpretative work of Clinical Competency Committees.
Med Educ. 2019;53:723-734.
https://onlinelibrary.wiley.com/doi/full/10.1111/medu.13884
. 2020.
21. Rojek AE, Khanna R, Yim JWL, et al. Differences in narrative language in
evaluations of medical students by gender and under-represented minority
status. J Gen Intern Med. 2019;34(5):684-691.
https://link.springer.com/article/10.1007%2Fs11606-019-04889-9
. 2020.
22. Ross FJ, Metro DG, Beaman ST, et al. A first look at the Accreditation
Council for Graduate Medical Education Anesthesiology Milestones:
Implementation of self-evaluation in a large residency program. J Clin
Anesth. 2016;32:17-24.

31
https://www.sciencedirect.com/science/article/abs/pii/S0952818016000477?
via%3Dihub. 2020.
23. Salles A, Awad M, Goldin L, et al. Estimating implicit and explicit gender
bias among health care professionals and surgeons. JAMA Netw Open.
2019;2(7):e196545.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2737309
.
2020.
24. Santen SA, Yamazaki K, Holmboe ES, Yarris LM, Hamstra SJ. Comparison
of male and female resident Milestone assessments during emergency
medicine residency training: A national study. Acad Med. 2020;95(2):263-
268. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7004441/
. 2020.
25. Saposnik G, Redelmeier D, Ruff CC, Tobler PN. Cognitive biases
associated with medical decisions: a systematic review. BMC Med Inform
Decis Mak. 2016;16(1):138.
https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911
-016-0377-1. 2020.
26. Schwind CJ, Williams RG, Boehler ML, Dunnington GL. Do individual
attendings’ post-rotation performance ratings detect residents’ clinical
performance deficiencies? Acad Med. 2004;79(5):453-457.
https://journals.lww.com/academicmedicine/Fulltext/2004/05000/Do_Individ
ual_Attendings__Post_rotation.16.aspx. 2020.
27. Surowiecki J. The Wisdom of Crowds. New York, NY: Anchor Books; 2005.
28. Teherani A, Hauer KE, Fernandez A, King TE Jr, Lucey C. How small
differences in assessed clinical performance amplify to large differences in
grades and awards: A cascade with serious consequences for students
underrepresented in medicine. Acad Med. 2018;93(9):1286-1292.
https://journals.lww.com/academicmedicine/fulltext/2018/09000/How_Small
_Differences_in_Assessed_Clinical.16.aspx. 2020.
29. Thomas MR, Beckman TJ, MauckKF, Cha SS, Thomas KG. Group
assessments of resident physicians improve reliability and decrease halo
error. J Gen Intern Med. 2011;26:759-764.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3138588/
. 2020.

32
Part 5: Post-Meeting Activities: Feedback, Documentation, and Follow-Up
Feedback to the resident or fellow is an essential activity of the Milestones
assessment system. Research has clearly shown that feedback is one of the most
effective educational tools faculty members and programs have to help residents
and fellows learn and improve.
The Milestones should be used to help residents
and fellows develop action plans and adjustments to their learning activities and
curriculum. Feedback sessions should be conducted in person.
Program directors will have different processes within their programs based on
program size. Some program directors may provide feedback to residents/fellows
themselves. Others will delegate this responsibility to one or more of the CCC
members or a separate set of advisors. Research is clear that interpreting and
understanding multi-source performance data, as represented by the Milestones,
should be facilitated and guided by a trusted advisor working with a resident/fellow
over time. This relationship has been termed an ‘educational alliance’ that
strengthens the residents’/fellows’ ability to engage with the feedback provider in
reflecting on their own performance and incorporating feedback into a plan for
improvement. (Telio, 2015, Ramani, 2019) Feedback is most effective when
structured as an ongoing dialogue rather than a one-time transmission of
information. This process builds learners’ skills as Master Adaptive Learners
equipped to engage in lifelong learning. (Cutrer, 2017)
The faculty members providing feedback should be trained to serve in a coaching
role. Training entails building skills in discussing feedback, guiding reflection, and
creating learning plans. (Armson, 2019) A coach uses strategies to help residents
build on their strengths and address areas for improvement as part of their learning
experience. (Palamara, 2018) Similarly, residents should receive training about how
to maximize the benefit of a coaching relationship, including how to receive and use
feedback even when it may feel uncomfortable. (Deiorio, 2017)
There are many different models that can be used to provide feedback, like ADAPT
- Ask-Discuss-Ask-Plan Together (Appendix H), and R2C2 (Appendix I). (Fainstad,
2018; Sargeant, 2018) Regardless of the particular model used by a program, the
basic features of high-quality feedback include:
1. Timeliness: The results of CCC deliberations and Milestones determinations
should be shared with the individual resident or fellow soon after the meeting
has occurred.
2. Specificity: The Milestones help to facilitate this criterion by providing
descriptive narratives. However, as noted above, the Milestones do not
represent the totality of a discipline, and many other important points of
feedback will likely arise in a CCC meeting that should also be captured and
shared with the individual resident or fellow. Generalities (often called “minimal”
feedback), such as “you’re doing great,” or, “should read more,” are not helpful
in promoting professional development, especially in the context of Milestones
data.
3. Balance reinforcing (“positive”) and corrective or constructive
(“negative”) feedback: It is important to include both in specific terms. An
imbalance between too much reinforcing or conversely corrective feedback can
undermine the effectiveness. The popular feedback sandwich (positive-

33
negative-positive) is not actually very effective and not routinely recommended.
Models for giving feedback are provided in Appendix H (ADAPT model) and
Appendix I (R2C2).
4. Learner reaction and reflection: It is very important to allow the individual
resident or fellow to react to and reflect on the feedback and Milestones data.
The two models provided below are excellent ways to facilitate this process.
Reaction and reflection help garner resident/fellow buy-in and development of
individualized learning plans (ILPs). Residents should be strongly encouraged,
in partnership with a faculty advisor and coach, to create their own ILP every six
months.
5. ILPs: Creating and executing an ILP after Milestones review is critical to
professional development and is often neglected in feedback. As Boud and
Molloy (2013) argue, feedback hasn’t occurred until the learner has actually
attempted an action or change with the information. Feedback is more than just
information giving and dissemination. (Lockyer, 2017)
6. Feedback should start with where the resident/fellow was at the last feedback
meeting and a review of the action plans created then.
CCCs should also provide feedback to the Program and the Program Evaluation
Committee as to which Milestones have been easier to assess based upon the
assessments presented. This feedback is critical for the program to improve its
curriculum (where the content of the milestone is taught) and where and how it is
assessed.
References:
1. Armson H, Lockyer JM, Zetkulic M, Könings KD, Sargeant J. Identifying
coaching skills to improve feedback use in postgraduate medical education.
Med Educ. 2019;53(5):477-493.
https://onlinelibrary.wiley.com/doi/full/10.1111/medu.13818. 2020.
2. Boud D, Molloy E. Feedback in Higher and Professional Education. 1st ed.
Sydney: Routledge; 2013.
3. Cutrer WB, Miller B, Pusic MV, et al. Fostering the development of master
adaptive learners: A conceptual model to guide skill acquisition in medical
education. Acad Med. 2017;92(1):70-75.
https://journals.lww.com/academicmedicine/Fulltext/2017/01000/Fostering_the_
Development_of_Master_Adaptive.24.aspx. 2020.
4. Deiorio N, Hammoud M. Coaching in Medical Education: A faculty handbook.
https://www.ama-assn.org/system/files/2019-09/coaching-medical-education-
faculty-handbook.pdf. 2020.
5. Fainstad T, McClintock AA, Van der Ridder MJ, Johnston SS, Patton KK.
Feedback can be less stressful: Medical trainee perceptions of using the
prepare to ADAPT (Ask-Discuss-Ask-Plan Together) Framework. Cureus.
2018;10(12):e3718. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6428363/.
2020.
6. Lockyer J, Carraccio C, Chan MK, et al. Core principles of assessment in
competency-based medical education. Med Teach. 2017;39(6):609-616.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1315082?journal
Code=imte20. 2020.
7. Palamara K, Kauffman C, Chang Y, et al. Professional development coaching
for residents: Results of a 3-year positive psychology coaching intervention. J
34
Gen Intern Med. 2018;33(11):1842-1844.
https://link.springer.com/article/10.1007%2Fs11606-018-4589-1
. 2020.
8. Ramani S, Könings KD, Ginsburg S, van der Vleuten CPM. Twelve tips to
promote a feedback culture with a growth mind-set: Swinging the feedback
pendulum from recipes to relationships. Med Teach. 2019;41(6):625-631.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2018.1432850?journal
Code=imte20. 2020.
9. Sargeant J, Lockyer JM, Mann K, et al. The R2C2 Model in residency
education: How does it foster coaching and promote feedback use? Acad Med.
2018;93(7):1055-1063.
https://journals.lww.com/academicmedicine/fulltext/2018/07000/The_R2C2_Mo
del_in_Residency_Education__How_Does_It.30.aspx. 2020.
10. Telio S, Ajjawi R, Regehr G. The "educational alliance" as a framework for
reconceptualizing feedback in medical education. Acad Med. 2015;90(5):609-
614.
https://journals.lww.com/academicmedicine/fulltext/2015/05000/The__Educatio
nal_Alliance__as_a_Framework_for.21.aspx. 2020.
35
Part 6: Legal Issues
The CCC can be an extremely beneficial structure to support legal constructs
required for academic decision-making. There are two Supreme Court decisions
that provide the context and framework for academic due process, including the
concept of a Clinical Competency Committee (See Key Legal Cases Supporting
Professional Judgment in GME).
Academic due process consists of three components:
1. notice (of deficiencies); and,
2. opportunity to cure; and,
3. a careful and deliberate decision-making process.
“Notice” and “Opportunity to Cure” are the heart of academics. Continuously,
residents and fellows are receiving feedback about how they might approach their
roles as clinicians, diagnosticians, and educators, in a way that is enhanced. This
notice may come in the form of routine feedback at the bedside, during rounds, in a
meeting, or in a structured assessment or evaluation process. Notice, or feedback,
can be formal or informal; verbal or written. An opportunity to cure simply
recognizes time following that feedback for the learner to demonstrate improvement
and change. An opportunity to cure may be a short period of time (even
immediate), or a more prolonged period (weeks or months), depending on the issue
at hand.
The CCC can serve as all, or part, of the ‘reasonable decision-making process.’ In
both Missouri v. Horowitz (“Horowitz”) and Michigan v. Ewing (“Ewing”), the faculty
evaluation committee was identified as being a core component of the reasonable
decision-making process; specifically, the cases reference “a regularly called
meeting of the faculty for the purpose of discussing student (resident/fellow)
performance.” While not specifically referred to at the time of the decision as the
“CCC,” this structure of a faculty committee is the legal construct supporting the
importance of what is now referred to as a CCC in today’s evaluation systems in
medicine. The Ewing case further supported the idea that a faculty decision-making
committee providing academic performance decisions that are conscientious and
made with careful deliberation (i.e., not arbitrary or capricious) constitutes
reasonable decision-making. When making academic decisions regarding
resident/fellow performance, promotion, or dismissal, the CCC provides a structure
recognized by the highest court in academic cases.
Reasonable decision-making processes should include all available information on
the learner’s performance, including “notices” and “opportunities to cure.” This
includes both verbal and written feedback, structured and unstructured
observations of performance, solicited and non-solicited feedback from others, and
any other information helpful to a careful decision-making process.
Documentation
When defending a legal case, contemporaneous documentation of events, actions,
or conversations are very helpful for confirming whether something actually
happened. Although there is no law requiring evaluations or performance feedback
to be in writing, the ACGME requires written rotational evaluations and semi-annual
36
evaluations of performance. Of course, it is natural within an academic clinical
setting that a faculty member provides a resident/fellow with routine verbal
feedback. Although it is not recorded, this verbal feedback also constitutes notice
and opportunity to cure (Horowitz).
While it is always helpful to have written performance documentation, lack thereof
should not deter evaluators from doing the right thing and using this information as
part of the overall evaluation process. One critical role of the CCC is to elicit
feedback from faculty members regarding performance in a variety of settings and
situations, and for the faculty to discuss performance based on individual
experiences and opinions. In many situations, this discussion at the CCC may be
the first time that issues emerge and indicate a pattern of performance or behavior.
This discussion is the heart of the CCC and should not be discounted just because
there is not a rotational evaluation or other assessment tool or form to support the
discussion. Research shows that the discussion among the faculty members in the
CCC often provides more accurate and robust information regarding learner
performance than the written evaluation alone, which may not represent a complete
view of actual performance. In fact, Schwind et al. demonstrates that verbal
discussion of actual performance is more accurate than what is provided in the
written evaluations. (2004)
These discussions are not only valuable to the formation of individual performance
evaluations, but also to demonstrate a “fair and reasonable decision-making
process” by the program.
The documentation of the CCC meeting itself can be one of the most valuable
documents to an institution when defending a resident/fellow dismissal or adverse
action. The ACGME does not have a requirement as to how the CCC meeting
should be documented, however, many programs will find it worthwhile to retain
minutes of CCC meetings. These minutes may be:
1. A written document reflecting the discussion of each resident’s/fellow’s
performance.
2. A concise summary of each resident’s/fellow’s performance and any action
or follow-up items.
3. Confidential (i.e., not shared with anyone other than the resident/fellow,
CCC, and program leadership).
4. Archived in accordance with the institution’s document retention policy in
consultation with legal counsel.
Some institutions may prefer #1 to be brief and use the Milestones reported to the
ACGME as #2.
Decision Process
The ACGME requires the CCC to make recommendations on resident/fellow
performance to the program director for review and action; thus, the program
director, and not the CCC, is the final decision maker. Still, in most situations, the
feedback and consensus of the CCC is critical in informing the program director of
the faculty’s expert opinion regarding progress and promotion.
37
In general, discussions of the CCC should lead to a “consensus” decision. That is,
after presentation of all data, and engagement of the members in a discussion of
their experience with, and opinion regarding the progress of a resident/fellow, the
Milestones assessment will be reached by consensus.
Nevertheless, the CCC may find a situation in which strongly held differing opinions
that are not modified through discussion fail to result in consensus. The Chair must
recognize and be prepared for these circumstances and appreciate their value. In
fact, these differences of opinion are crucial to authentic assessment, and another
opportunity to discuss the opinions provided. Govaerts et al. (2019) remind us that
such tensions are inherent in competency-based education (assessment of learning
versus assessment for learning; formative versus summative assessment) and
suggest the integration of Polarity Thinking
TM
as one mechanism.
The CCC members should discuss the possibility of disagreement at the outset and
should consider describing how they will proceed. Although a written description of
the CCC is not required, it may be useful for the CCC to describe its processes to
clarify them for one another, and to help communicate to the residents/fellows and
other faculty members. The ACGME provides no specific guidance in this setting.
The committee should establish its own policy and apply it consistently, taking into
account input from the designated institutional official (DIO) and Legal office. While
it is recognized that decisions regarding actions such as remediation, probation,
and promotion can be difficult and programs may resort to voting, the ACGME and
the authors of this Guidebook strongly discourage voting as a decisional approach.
As the Milestones are designed to guide a developmental judgment, CCCs should
not vote on individual sub-competencies and milestones. If programs do choose to
use voting, it is very important to be clear about what exactly the vote means from
the outset, and to ensure that the process of voting does not provide a false sense
of power to the committee. For example, is a vote being taken to determine if
performance is not at an expected competence level, or is the vote to recommend a
disciplinary action, remediation, or dismissal? If a vote is held and there is a narrow
result, (e.g., four to three), the program director’s expert decision on a
resident/fellow may seem less clear cut if the resident/fellow subsequently appeals.
Regardless of whether a vote is taken, the CCC must remember that the decision
of the committee is advisory to the program director, and the program director has
the responsibility to be the final decision maker. With these mechanisms in place
and followed, fundamental fairness to both residents/fellows and committee
members is provided, and challenges to process consistency and fairness are
prospectively addressed.
Peer-Review Privilege
Peer-review statutes fall under state law, and thus vary from state to state. In
general, peer-review privilege has some common tenets that generally do not apply
to CCCs and resident/fellow performance evaluation.
Generally speaking, peer-review privilege:
● protects discussion of clinical performance for the purpose of internal quality
assessment, not evaluation and decisions communicated to external parties;
38
and,
● applies to in-person meetings where the information is maintained internally,
not communicated outside of the peer-review process (e.g., to clinical
advisors, other departments, or external agencies).
Each institution should review its peer-review statute with its legal counsel to
determine if it should be applied to the CCC. Likewise, given the ever-changing
legal environment and number of cases being heard regarding resident
performance, an institution’s legal counsel should regularly review new case law
and decisions in the state for updated rulings and orders issued by courts.
Notwithstanding a program’s natural tendency to want to maintain strict
confidentiality, if conducted in accordance with these guidelines, the discussions
and recommendations of the CCC are generally helpful when defending a
program’s decision to dismiss a resident/fellow (see Horowitz and Ewing). Carefully
prepared CCC minutes can provide one of the strongest legal defenses to support
dismissal actions by demonstrating the three core tenants of academic due
process: notice of deficiencies; opportunity to cure; and a reasonable decision-
making process.
The ACGME has been very clear that the Milestones are not intended for non-
residency (or fellowship) use. They are not used by the American Board of Medical
Specialties member certifying boards or by the certifying boards of the American
Osteopathic Association for specialty board certification. “The ACGME does not
have evidence that individual Milestones data
can be validly used in any other
context beyond provision of individual resident and fellow feedback, especially for
any higher stakes decisions,” such as licensure. The ACGME assumes that most
state medical licensing boards (including osteopathic medical boards) heed the
ACGME declaration that the Milestones are not designed for any non-GME
program use. In April 2018, the ACGME released a position paper, “Use of
Individual Milestones Data by External Entities for High Stakes Decisions - A
Function for Which they Are not Designed or Intended,” which describes the
potential adverse consequences if the Milestones are used by external entities.
Appeals and Due Process
The members of the faculty must be encouraged to provide candid and robust
evaluations that are reflective of actual performance. Evaluations are based on
each faculty member’s observations, judgments, and expectations. A faculty
member should complete evaluations in an honest and good-faith effort to provide
feedback to the resident/fellow with the goal of identifying both strengths and
deficiencies, in order to help the resident/fellow to improve academic performance.
Programs should be aware that allowing residents/fellows to appeal performance
evaluations (rotational evaluations, semi-annual evaluations, etc.) can send a
message to the residents/fellows that faculty member or program director feedback
is negotiable. It can also suggest to faculty members and program directors that
their feedback, usually critical, can be subject to scrutiny and overturned if a
resident/fellow complains. Programs should discuss with legal counsel the impact
of allowing residents/fellows to appeal performance evaluations or academic
evaluation decisions. Most institutions do not allow due process for routine
39
feedback, including assessment and evaluations, and the ACGME does not require
it for these purposes.
The ACGME does encourage programs using progressive disciplinary processes
(probation) to allow these actions, as well as termination or non-promotion,
resulting from CCC decisions to be eligible for appeal to ensure the department and
institution follow the policies in place regarding the decision-making process.
Key Legal Cases Supporting Professional Judgment in GME
University of Missouri v. Horowitz (1978)
Board of Curators of Univ. of Mo. v. Horowitz, 435 U.S. 78, 98 S. Ct. 948, 55 L. Ed.
2d 124 (1978).
Case Summary: Ms. Horowitz excelled in her first two years of medical school, but
received criticism from the faculty as she began her clinical rotations. She was
provided feedback in her rotational evaluations regarding her attendance, slovenly
appearance, hygiene, and bedside manner. Despite feedback, Ms. Horowitz’s
behavior did not improve. The school’s faculty evaluation committee ultimately
recommended her dismissal from medical school. Ms. Horowitz appealed the
decision to the Dean. The Dean allowed Ms. Horowitz the opportunity to be
evaluated by seven independent physicians. At the conclusion
of the rotations, the faculty provided feedback to the Dean of varied opinion.
Based on the feedback of the independent faculty evaluators, the Dean upheld the
dismissal decision. This case and the issue of academic due process were
ultimately argued in front of the Supreme Court. The Court supported the
University’s decision based on the following:
● Ms. Horowitz was provided notice of her deficiencies through private verbal
feedback and her rotational evaluations.
● Ms. Horowitz was provided an opportunity to cure her deficiencies.
● The decision was made carefully and deliberately. The regularly called
meeting of the faculty, called for the purpose of evaluating academic
performance, was noted as being a reasonable decision-making process
consisting of faculty members, expected to evaluate student performance.
● The Court decision noted that under this particular set of circumstances the
rotation with the seven physicians was much more process than was due.
University of Michigan vs. Ewing, (1985)
Regents of Univ. of Mich. v. Ewing, 474 U.S. 214, 106 S. Ct. 507, 88 L. Ed. 2d 523
(1985).
Case Summary: Mr. Ewing was enrolled in the six-year BS/MD program. After four
years, he was eligible to write the NBME Step 1 exam. Mr. Ewing failed the exam
and was subsequently dismissed from medical school. He sued, citing at least 11
other students who failed the exam and were allowed to stay enrolled in school and
retake the test; some were allowed to retake the exam three and four times. The
decision to dismiss Mr. Ewing was made by the faculty committee charged with
reviewing academic performance. This committee reviewed Mr. Ewing’s entire
academic record and determined that based on his overall performance (including
several incompletes, required repeats of courses, and the lowest score ever
recorded on the NBME exam at this school), he did not have the ability or aptitude
required of a physician and had no chance of succeeding. The Court sided with the
school noting:

40
1. “The narrow avenue for judicial review of the substance of academic
decisions precludes any conclusion that such decision was a substantial
departure from accepted academic norms as to demonstrate the faculty did
not exercise professional judgment.”
2. The decision was “conscientious and made with careful deliberation,” citing
the regularly called faculty meeting structure, and the Promotion and
Review Board.
3. The faculty rightly reviewed Mr. Ewing’s entire academic record, not just a
single test, rotation, or incident, to provide context to the decision.
References
1. ACGME. Use of Individual Milestones Data by External Entities for High
Stakes Decisions - A Function for Which they Are not Designed or Intended.
https://www.acgme.org/Portals/0/PDFs/Milestones/UseofIndividualMilestones
DatabyExternalEntitiesforHighStakesDecisions.pdf?ver=2018-04-12-110745-
440. 2020.
2. Govaerts MJB, van der Vleuten CPM, Holmboe ES. Managing tensions in
assessment: moving beyond either-or assessment. Med Educ.
2019;53(1):64-75.
https://onlinelibrary.wiley.com/doi/full/10.1111/medu.13656
. 2020.
3. Schwind CJ, Williams RG, Boehler ML, Dunnington GL. Do individual
attendings’ post-rotation performance ratings detect residents’ clinical
performance deficiencies? Acad Med. 2004;79(5):453-457.
https://journals.lww.com/academicmedicine/Fulltext/2004/05000/Do_Individu
al_Attendings__Post_rotation.16.aspx. 2020.
41
Part 7: Other Uses for the CCC
Although the primary role of the CCC is that of documenting residents’/fellows’
performance on the Milestones, by virtue of their review and synthesis of a vast
array of assessment data from different learning experiences, CCCs are uniquely
qualified to render judgements not only on resident/fellow performance, but on the
curriculum and the quality of the assessment system. CCCs can play many
important roles in the assessment system, including:
1. Assessing transferring residents/fellows
2. Contributing to the Annual Program Evaluation
4. Faculty development
5. Quality improvement of the assessment system
6. Assisting the institutional Graduate Medical Education Committee (GMEC)
7. Continuous educational quality improvement
8. Simplifying a program’s individual and collective assessment tools
In this section, we describe an expansion of the role of the CCC outlined in the
Common Program Requirements in order for programs and institutions to make the
most of these committees’ important work.
Transfers/Admittance from Non-ACGME-Accredited Programs
When residents/fellows transfer into an ACGME-accredited program with previous
experience from a non-ACGME-accredited program, an assessment on the
Milestones is required within 12 weeks of matriculation. Programs should also
review the resident’s/fellow’s Milestones results from the previous program when
applicable. The CCC may be used to assess the competence of those
residents/fellows who are either transferring into a program from a period of prior
education or applying to a fellowship with core residency education experience from
a non-ACGME-accredited program.
Annual Program Evaluation
Through the process of reviewing vast amounts of resident/fellow assessment data,
CCCs should take the time to develop “Milestone maps” (i.e., a spreadsheet to
track where each milestone is taught and assessed). CCCs can use these maps to
determine the extent of the curricular content for each milestone, including the
teaching and assessment methods and the learning experiences where the
material is currently taught and/or assessed, or perhaps where it should be
taught/assessed. This process can illuminate any potential gaps or redundancies in
the curriculum. Then, CCCs can make recommendations for the development of
new rotations or learning experiences that may help address curricular concerns.
Such information can be formally submitted to the program director at least once
per year to be included on the agenda for the Program Evaluation Committee
(PEC) as it performs the Annual Program Evaluation. The PEC is expected to
review multiple data points during this review, including information about the
curriculum and aggregate Milestones data.
42
Faculty Development
CCCs review an inordinate amount of faculty ratings and narratives about
residents’/fellows’ performance and must make important decisions based on this
data. Thus, they can provide important insights on the usefulness of such data and
offer feedback to be used for the purpose of faculty development. Program
directors are expected to review the performance of their faculty members at least
annually, including providing faculty members with feedback on their evaluations.
The CCC can have a significant role in this key faculty development mission.
Faculty development is needed at three levels: 1) the program director; 2) the
engaged core and other faculty members who join the CCC; and, 3) the faculty
members “in the trenches” who may not be as fully involved in educational
programming or administration, but who have essential roles in actively teaching
and assessing residents/fellows. Each group will have different needs. Program
directors and CCC members will need a deeper understanding of the Milestones,
assessment, group process, and program evaluation. Faculty members need to
understand what key elements of assessment information they need to contribute
to the larger picture of each resident/learner.
Faculty professional development is a required program component. The ACGME
recognizes that although “evaluation is a core faculty competency… most [faculty
members] will need additional training in [the] evaluation process,” to include
evaluation process training (how to interpret aggregated evaluation data),
understanding how many assessments are needed for each Milestone, assurance
of data quality, and application of QI methods to the evaluation processes. The
CCC provides an opportunity for faculty development for other program faculty
members as well: to understand the CCC process and how its evaluations of
residents/fellows fit into the overall assessment of resident/fellow performance
using the Milestones.
Quality Improvement
In aggregate, CCCs can review not only assessment data generated by the core
faculty members, but also their own Milestones ratings. Using aggregate reports
from their residency management system, CCCs can review trends in the ratings
for specific milestones and initiate conversations to assist in explaining such trends.
For example, if most PGY-2s are scoring low on the practice-based learning and
improvement milestones, there can be multiple reasons for this finding. This may be
due to lack of data, inadequate data, inadequate performance, or perhaps
inadequate sampling of performance. In some situations, there may be no
assessment data at all for certain milestones. This finding may also signal gaps in
the curriculum, a lack of assessment, inadequate documentation, and presentation
of assessment data to the CCC or some combination thereof. Mechanisms should
be put in place to recognize these issues and attempts should be made to address
them prior to the next review cycle.
Assist the GMEC
The CCC can assist the GMEC in the oversight of the effectiveness of programs’
curricula by providing the aggregate Milestones data for each program and trends

43
in the data, and by making recommendations for programs’ Annual Program
Evaluations. Per the Institutional Requirements, the GMEC’s responsibilities must
include oversight of:
“the quality of educational experiences in each ACGME-accredited
program that lead to measurable achievement of educational outcomes as
identified in the ACGME Common and specialty-/subspecialty-specific
Program Requirements;”
(Outcome)
“the ACGME-accredited program(s)’ annual program evaluations and self-
studies;”
(Core)
Continuous Educational Quality Improvement
For the individual resident/fellow, the CCC offers insights and perspectives from a
group of faculty members, and comparison of an individual’s performance to a
national standard, the Milestones. For the entire program, the CCC serves as an
early warning system if a resident/fellow fails to progress, and therefore identifies
an opportunity for remediation. For the members of the faculty, CCCs can be an
opportunity to balance out the “hawks” and “doves,” and to develop a more
standardized, consistent, explicit approach to expectations of resident/fellow
performance. More importantly, through longitudinal dialogue and repeated
sessions, faculty members can develop a better shared mental model of
competence and reduce the variability in assessment judgments.
Simplify a Program’s Individual and Collective Assessment Tools
The CCC can identify which assessments are most useful, and where there are
gaps. A program may be able to eliminate administrative burden. It may not be
feasible or even necessary for faculty members to complete multi-page evaluation
forms, for example. As stated earlier, the true assessment instrument is not the tool
or form, it is the faculty member(s) or others using it. CCCs can help to identify
barriers and impediments to effective faculty members’ evaluations and create
faculty development or other intervention opportunities.
References:
1. ACGME. ACGME Common Program Requirements (Residency).
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResiden
cy2019.pdf. 2020.
44
Part 8: Individualized Learning Plans and Final Evaluations: The Other Roles
of the CCC
The CCC has two other critically important roles that are core requirements for the
program.
1) The program director/designee, with input from the CCC, must: “assist
residents in developing individualized learning plans to capitalize on their
strengths and identify areas for growth” (Program Requirement V.A.1.d).(2)
and,
2) The ACGME-required final evaluation for each resident, completed by the
program director upon each resident’s program completion, must “consider
recommendations from the Clinical Competency Committee”
V.A.2.a).(2).(c)
Individualized Learning Plans (ILPs)
Learning contracts are “without question the single most potent tool I have come
across in my more than half-century of experience with adult education.”
(Knowles,1990)
Adult learning theory is premised on the construct that adults learn best when they
are actively engaged in the learning process and self-direct their own learning goals
and activities. (Knowles, Holton and Swanson, 2005). The ACGME Common
Program Requirements now reference ILPs [Common Program Requirements
V.A.1.d.(1)-(3)]: “The program director (or designee) must… assist residents in
developing individualized learning plans to capitalize strengths and identify areas of
growth.”
At the point of graduation, program directors must certify that each resident has
achieved competence as an independent, self-directed, and lifelong learner. The
Core Competency of Practice-Based Learning and Improvement is a fundamental
component of this certification. Self-directed learning is a process by which
individuals identify and/or acknowledge their own learning needs, find resources to
meet those needs, and subsequently evaluate their own achievements; it is integral
to maintaining professional competence. An ILP is also an important tool for the
struggling resident or fellow.
Although the ACGME expects all residents/fellows to have individual learning plans,
often CCCs and program directors only think about using them in for those learners
who are performing below expectations. Residents/fellows struggling to perform at
acceptable standards are often a source of frustration for faculty members and for
CCCs. When the CCC and/or the faculty acknowledge that a learner is not meeting
academic standards, there is sometimes hesitation regarding a path forward. Often,
this hesitation stems from learners who are perceived as lacking insight to their own
deficiencies. In addition to being unable to self-reflect on performance, these
learners also tend to disregard faculty members’ feedback (often perceived as
biased or misdirected), claim that the faculty members have not adequately taught
them or provided them with helpful feedback, and cannot acknowledge their own
personal role and responsibility in the learning process. But the inability to
accurately “self -assess” and have appropriate insight is almost universal among
those performing poorly; program directors and faculty members should expect it
45
and not be surprised by it. Indeed, the very lack of insight that makes
residents/fellows incapable of recognizing their own poor performance, frequently
makes it nearly impossible for them to succeed with a remediation plan.
An ILP should be formulated by the learner for the learner, and should include
personal learning objectives, as well as resources and strategies to achieve them.
While the learner should be able to create an initial ILP, the ILP content should be
guided by a facilitator (faculty member, advisor, coach, or program director). The
draft ILP created by the resident/fellow can provide enormous insight to the
program director and/or CCC; the information contained in the ILP is one way to
determine if the learner has the ability to self-reflect based on feedback received,
and the insight required to be successful in remediating. Those unable to “own”
their deficiency(ies) and construct or at least contribute in a major way to a plan to
address it, are unlikely to be successful.
Creating an ILP should actively engage learners to take ownership of their own
learning. (Li & Burke, 2010) ILPs allow the learner to focus on priority areas, re-
evaluate learning needs, and have regular discussions about achieving learning
goals.
Components of an ILP (Li & Burke, 2010):
1. Reflection on goals and self-assessment of strengths and weaknesses
2. Generation of specific learning goals and/or objectives
3. Specific plans or strategies to achieve each goal focused on what the
learner will do to improve
4. Mutual agreement on how the assessment of progress on each goal will be
determined
5. Eventual revision of goals or creation of new goals based on performance
6. Expected timeline
ILPs ARE:
• Formulated by the individual (resident/fellow) – made by the learner, for the
learner
• Guided by a facilitator (faculty member, advisor, coach, or program
director)
• An exercise in self-assessment and self-reflection
• Iterative
• An ACGME core requirement
• An indicator of insight and ability to become an independent lifelong learner
ILPs are NOT:
• Set in stone – they can and should be revisited by both the learner and the
facilitator
• A portfolio
• Evaluations
• The sole or major responsibility of the program director (or faculty) or the
program
CCCs do not “create” ILPs. This is the work of the residents/fellows, co-produced
with the program director (or designee), an advisor, or coach.

46
The Final Evaluation
Upon completion of a program, the program director must provide a final evaluation
for each resident/fellow (Common Program Requirement V.A.2.). In the past, this
was often referred to as the “Final Summative Evaluation.” While this evaluation
has been a perfunctory document and process for residents/fellows successfully
completing a residency or fellowship and progressing to the next stage of their
career, the final evaluation for residents/fellows who depart the program prior to
completion, typically for performance reasons, are even more important and can be
difficult to write.
The ACGME requires that the “specialty-specific Milestones, and when applicable
the specialty-specific Case Logs, must be used as tools to ensure residents are
able to engage in autonomous practice upon completion of the program” [Program
Requirement V.A.2.a).(1)]. The complete requirements for the final evaluation
(Common Program Requirement V.A.2.) are listed in Table 5 below.
When a resident/fellow is dismissed from the program, or resigns early due to
performance concerns, the final evaluation becomes the document of record
regarding the resident’s/fellow’s achievement to date in each of the Core
Competencies. It also describes areas in which the resident/fellow is either deficient
or has not attained a level of performance consistent with PGY level expectations.
Additionally, the final evaluation can contain important contextual information,
including the dates of enrollment in the program, any relevant prior
education/training information, description of any behavioral issues or concerns,
and a summary paragraph describing the program director’s overall impression of
the individual resident/fellow, their achievements, any ongoing concerns, or areas
for future focus. For residents and fellows in procedural specialties, the final
evaluation may also include a summary of procedural cases performed at the
institution.
Table 5: Common Program Requirements for the Final Evaluation (previously
the Final Summative Evaluation)
V.A.2.a)
be provided by the program director for each resident upon completion
of the program
V.A.2.a).(1)
specialty-specific Milestones, and when applicable the specialty-specific
Case Logs, must be used as tools to ensure residents are able to
engage in autonomous practice upon completion of the program
V.A.2.a).(2).(a)
become part of the resident’s permanent record maintained by the
institution, and must be accessible for review by the resident in
accordance with institutional policy
V.A.2.a).(2).(b)
verify that the resident has demonstrated the knowledge, skills, and
behaviors necessary to enter autonomous practice
V.A.2.a).(2).(c)
consider recommendations from the Clinical Competency Committee

47
V.A.2.a).(2).(d)
be shared with the resident upon completion of the program
The final evaluation should be a comprehensive, stand-alone document that
encompasses the scope of a resident’s/fellow’s performance while enrolled in the
program. The final evaluation should not be confused with a letter of
recommendation, which is typically prepared to promote or support an individual
with a positive bias. Instead, the final evaluation should be written with candor, in a
way that is fair and balanced with regard to actual performance.
The final evaluation can be an important tool for a program receiving an off-cycle
resident/fellow. If properly written, the program receiving the resident/fellow should
be able to use the final evaluation from the prior program to ascertain the
resident’s/fellow’s current performance level for each Core Competency,
understand the resident’s/fellow’s strengths and weaknesses, understand the
context in which the resident/fellow departed the prior program, and provide
continuity of education, supervision, and feedback.
The final evaluation is also valuable for well performing residents as transitioning
from residency to fellowship or into their first post-GME professional role.
The final evaluation SHOULD be:
• Sufficiently comprehensive to stand alone in the resident or fellow’s
permanent record as an historic document of enrollment, achievement, and
areas of concern
• Honest – fair and balanced
• Competency-based, including knowledge, skills, and behaviors
• Signed and dated by the program director
• Maintained in the permanent academic record of the program and/or
institution
• Provided to the resident/fellow when finalized and signed
• Provided to others upon request (as appropriate, and when indicated, with
the approval of the resident/fellow)
The final evaluation SHOULD NOT:
• Misrepresent actual performance in any way
• Serve as a letter of recommendation
• Be negotiated by the resident/fellow or anyone else (the content of the final
evaluation must be the program director’s honest view of performance at
the conclusion of the resident’s/fellow’s time in the program
Some programs ask departing residents/fellows to sign the final evaluation retained
for their permanent file.
The Milestones were not designed to be used for this purpose, and the authors of
this guidebook strongly recommend that programs NOT substitute the final
Milestones Report submitted to the ACGME for this final evaluation document.

48
The authors recommend contacting the Sponsoring Institution’s DIO to learn if the
program should also collaborate with the institutional Legal and/or Human
Resources entities for guidance.
Conclusion
Although CCCs do not create ILPs or final evaluations, they have critical input into
these important, required program processes. As such, they benefit from
understanding how their judgement of resident/fellow progress will be used by the
program director beyond Milestones ratings alone.
References:
1. ACGME. ACGME Common Program Requirements.
https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResiden
cy2019.pdf. 2020.
2. Knowles M. The Adult Learner: A Neglected Species. Houston, TX: Gulf Pub
Co; 1990.
3. Knowles MS, Holton EF III, Swanson RA. The Adult Learners: The Definitive
Class in Adult Education and Human Resources Development. 6th ed.
Burlington, MA: Elsevier; 2005.
4. Li ST, Burke AE. Individualized learning plans: basics and beyond. Academic
Pediatrics. 2010;10(5):289-292.
https://linkinghub.elsevier.com/retrieve/pii/S1876-2859(10)00196-8
. 2020.
49
Part 9: Institutional Oversight of CCCs
[Acknowledgement to Y. Wimberly, MD, MSc, FAAP, Associate Dean of Clinical
Affairs and Designated institutional Official, Morehouse School of Medicine]
Although there are no CCC-specific requirements in the ACGME Institutional
Requirements, DIOs and their team, as well as the GMEC, have a critically
important oversight role in ensuring each program’s CCC processes adhere to the
Common Program Requirements. They may be a source of resources, including for
faculty development, and provide ways to share lessons learned among the
institution’s programs.
In addition, there is at least one institutional requirement that may impact CCCs.
The Sponsoring Institution is responsible for programs’ development of “promotion
criteria” and criteria for renewal of a resident’s/fellow’s appointment (Institutional
Requirement IV.C.), and those conditions for reappointment and promotion to a
subsequent PGY level must be in the contract or letter of appointment (Institutional
Requirement IV.B.2.d)). Many CCCs may de facto “act” as promotion committees
and apply their judgement of resident/fellow performance to recommend
resident/fellow renewal and promotion to the next program year. The Common
Program Requirements require “at least annually...a summative evaluation of each
resident that includes their readiness to progress to the next year of the program, if
applicable.” [Common Program Requirement V.A.1.e)] Although not stated
explicitly, it is likely that an effective CCC will have collaborated with the program
director to identify the promotion criteria or at the very least, align Milestones
performance with them. The CCC should inform the program director of its review
so that the program director can truly exercise the responsibility, authority, and
accountability for promotion of residents/fellows. [Program Requirement II.A.4.]
For residents not making sufficient progress, other institutional requirements will
likely become important, such as due process and grievance policies. Ideally the
Sponsoring Institution and its programs are closely aligned and the DIO and the
program directors are effective collaborators.
The GMEC may wish to monitor CCCs through their oversight of each program’s
Annual Program Evaluation and Self-Studies [Institutional Requirement I.B.4.a).(4)].
The GMEC may wish to make some aspect of the CCC’s assessments one of the
performance indicators used and reported as part of the institution’s Annual
Institutional Review (AIR).
One institution’s experience with this is described using change management
strategies and realizing effective engagement. (Dagnone, 2019)
Appendix H provides a checklist of important CCC elements for DIOs and GMECs
to use in their monitoring. It can be modified to reflect program-/institutional-specific
practices. It outlines potential expectations for the DIO and GMEC, the program
director, the CCC Chair, CCC members, program faculty members and evaluators,
and residents/fellows. It can be used to review the current status of CCCs within an
institution and to identify potential areas for improvement, enhanced resources, and
strategies to disseminate best practices.

50
References:
1. ACGME. ACGME Institutional Requirements.
https://www.acgme.org/Portals/0/PFAssets/InstitutionalRequirements/000Institut
ionalRequirements2018.pdf?ver=2018-02-19-132236-600. 2020.
2. Dagnone D, Stockley D, Flynn L. Delivering on the promise of competency
based medical education - an institutional approach. Can Med Educ J.
2019;10(1):e28-e38. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6445322/
.
2020.

51
Part 10: Current Research
The ACGME Department of Research, Milestone Development, and Evaluation
maintains a bibliography of research related to the Milestones and Clinical
Competency Committees. The bibliography is updated approximately every six
months and can be found at
https://www.acgme.org/What-We-
Do/Accreditation/Milestones/Research.

52
Appendix A: The High Performing Residency Assessment System
At the program level, residents/fellows are assessed routinely through a
combination of many assessment tools. These include: direct observations; global
evaluation; audits and review of clinical performance data; multisource feedback
from team members, including peers, nurses, patients, and family; simulation; in-
service training examinations (ITE); self-assessment; and others. Increasingly, the
Milestones and entrustable professional activities (EPAs) are used as a guiding
framework and “blueprint” for expected performance. Assessment tools are
selected intentionally to allow routine, frequent, formative feedback to the
resident/fellow to affirm areas of successful performance and to highlight those
aspects that need to be improved. The CCC is the committee that synthesizes
data—quantitative from in-service exams and clinical performance audits, and
qualitative from observers and co-workers. Using the Milestones, the committee
forms a consensus decision, or a judgment, regarding each resident’s/fellow’s
performance. The CCC provides those conclusions to the program director, who
makes the final determination on residents’/fellows’ Milestone “level” at least twice
yearly. These are provided to the applicable ACGME Review Committee and, in
some cases, the pertinent specialty boards. The ACGME’s unit of analysis is the
program, and the Review Committees use aggregate Milestones information
comparing a program with all accredited programs in the given specialty.
The comparison against these benchmarks serves as one source of input into the
ACGME’s determination of program quality and accreditation decisions. The unit of
analysis is the “individual” for certification and credentialing entities. Collectively, all
residents/fellows, faculty members/program directors/programs, the ACGME, and
certification and credentialing entities are accountable to the public for honest
assessments of residents’/fellows’ performance and truthful verification of their
readiness to progress to independent practice. Data (D) is essential for the entire
system to engage in continuous quality improvement, especially to create
meaningful feedback (FB) loops within the program and back to programs from the
53
ACGME. Programs and residents and fellows can currently download their
Milestones report after each reporting period.
54
Appendix B: CCC Quiz
1. Requirements for a CCC are found in:
A. The ACGME Common Program Requirements
B. The ACGME Institutional Requirements
C. The CLER Pathways to Excellence document
D. Both A and B
E. None of the above
2. Which of the following requirements of CCCs is an ACGME core requirement?
A. Include faculty members from other programs and non-physician
members of the health care team
B. Review all residents/fellows at least semi-annually
C. Have a written description of the CCC’s responsibilities
D. Allow residents/fellows to exercise a grievance process if they disagree
with the Milestone determination of the CCC
3. The minimum number of CCC members is:
A. 1
B. 2
C. 3
D. 4
E. As many as necessary so that all divisions/subspecialties must be
represented
F. None of the above; there are no specific requirements on the numbers
needed
4. Who of the following should ALWAYS chair the CCC?
A. Program director
B. Associate program director
C. Department Chair
D. DIO
E. Head, GMEC
F. Most senior faculty member on the committee
G. None of the above
5. The CCC must include:
A. Patients
B. Nurses
C. Peer-selected residents or fellows
D. Members of the program faculty
E. Program director
F. All of the above
G. None of the above
6. How many residents/fellows must participate on the CCC?
A. 0
B. 1
C. At least one peer-selected resident or fellow
D. At least one from every year of the program
E. At least one chief resident
55
7. CCC members:
A. Determine each resident/fellow’s progress on achievement of the
specialty-specific Milestones
B. Only consider residents/fellows who need remediation
C. Only review residents/fellows in their final year of the program
D. Review the decisions the program director has already made regarding
each resident/fellow and provide advice
E. Vote on each resident’s/fellow’s performance
8. The CCC must:
A. Submit Milestones summaries to the ACGME
B. Meet with all residents/fellows to discuss their individual progress on the
Milestones
C. Design and implement any remediation plan necessary (and mentor the
resident/fellow throughout)
D. Review all resident/fellow evaluations at least semi-annually
E. Share Milestones evaluations with the specialty board and state
licensing board
9. According to the ACGME, the minutes of the CCC must be:
A. Fully transcribed
B. Retained as a summary of all residents/fellows
C. Retained only as a summary of the sub-optimally performing
residents/fellows
D. Provided to the ACGME
E. None of the above
10. According to the ACGME, all residents/fellows must be able to exercise a
grievance/due process (“appeal”) if they disagree with the CCC regarding the
Milestones determination it plans to report to the ACGME.
A. True
B. False
C. It depends
11. Who makes the final decision on a resident’s/fellow’s Milestones level?
A. The CCC
B. The resident’s/fellow’s advisor
C. The resident/fellow
D. The ACGME
E. The program director
12. In order to serve on a CCC, a chief resident must:
A. Have completed the core program
B. Be in the last year of the core program
C. None of the above; a chief resident cannot be on a CCC
13. Program coordinators:
A. May serve as voting members of CCCs
B. Can manage submission of Milestones data for the ACGME
C. Should not attend the CCC meeting
D. Should participate as voting members of the CCC
56
E. None of the above
14. Which of the following is true about CCCs?
A. The best size of a CCC is 12-15 members
B. At least one peer-selected resident should attend
C. Faculty members and/or health professionals with “different”
voices/options are encouraged to participate
D. The most senior persons should express their opinion first
E. None of the above
15. The most reliable assessment of performance is:
A. Multiple choice (written) examination
B. Global end-of-rotation evaluation
C. Multi-rater evaluation (multisource feedback)
D. Procedural log
E. Oral examination
F. Observation of actual performance
16. The literature suggests the idea size of a CCC is:
A. 3 to 5
B. 5 to 7
C. 7 to 9
D. 9 to 11
E. None of the above
17. Which of the following statements regarding Milestones assessments is true?
A. Programs should give faculty members the entire Set of Milestones for
them to use as part of their end-of-rotation evaluations
B. Faculty members should be encouraged to make inferences on the
performance of residents ONLY based upon the performance they have
directly observed
C. Faculty members should generally use the Milestones level that
corresponds to a resident’s year in training (i.e., Level 1 for a PGY-1
resident)
D. Information gained from informal “hallway” conversations can be useful
E. CCCs should use the average calculated by their resident management
system to determine the Milestones level
18. Groupthink is a phenomenon that occurs when the desire for group consensus
overrides people’s common-sense desire to present alternatives, criticize a
position, or express an unpopular opinion. Which of the following is a risk for
groupthink?
A. The CCC feels pressure to make a consensus decision with inadequate
time (decisional stress)
B. Low level of group cohesion
C. Lack of a strong dominating leader
D. The CCC cultivates an environment that encourages dissent
19. A CCC member says, “this is a strong resident, and I think a 2.5 Milestone
rating is appropriate,” and provides two supporting vignettes. This is mostly
likely an example of which type of cognitive bias that is common in groups?
57
A. Authority bias
B. Anchoring bias
C. Framing bias
D. Confirmation bias
20. Using what’s known from the literature to encourage good group processes, the
CCC should:
A. Encourage the most senior person to discuss a resident/fellow first
B. Have the CCC chair state opinions first
C. Avoid a structured format and use open forum for discussion
D. Use only the synthesis of a resident’s/fellow’s performance rather than
the underlying data used to make that synthesis
E. Ask one member to offer an opposing or different view to help represent
all possible perspectives
21. Feedback to residents/fellows following the CCC meeting is best accomplished
through an email providing them with a written report of their Milestones
performance.
A. True
B. False
22. Individualized Learning Plans are required by the ACGME:
A. Only for residents/fellows failing to progress
B. All residents/fellows
C. Only residents/fellows in the first year of the program
D. Only residents/fellows in the final year of the program
23. An applicant is accepted through an “exceptional candidate” exception and
matriculates into the program. A performance evaluation by the CCC must take
place:
A. Within 2 weeks
B. Within 8 weeks
C. Within 12 weeks
D. Within 20 weeks
24. Which of the following is/are other possible roles of the CCC?
A. Contributing information for use in Annual Program Evaluation
B. Assessing the competence of residents/fellows transferring from non-
ACGME-accredited programs to ACGME-accredited programs
C. Faculty development for core faculty members
D. All of the above
E. None of the above
Modified from an earlier quiz presented by Andolsek, KM and Nagler, A at the
2013 ACGME Annual Educational Conference
58
Appendix B: Quiz Answers
1. A
2. B
3. C
4. G
5. D
6. A
7. A
8. D
9. E
10. B
11. E
12. A
13. B
14. C
15. F
16. B
17. D
18. A
19. B
20. E
21. B
22. B
23. C
24. D
59
Appendix C: Case Studies
Mini Case Studies/FAQs/Common Dilemmas/Challenging Situations/Promising
Practices
1. Program director, “Dr. C,” is an accomplished clinician and well-regarded
educator. Dr. C recruits several faculty members to the newly constituted CCC,
but decides to chair the committee to ensure everything occurs correctly and
meets ACGME expectations.
Program directors and programs should think carefully about the role of the
program director in the CCC. The American Board of Anesthesiology precludes the
program director from serving as chair. The other boards and the ACGME
are silent on this issue. Even if there are no rules, it is worthwhile to think through
the role of the program director on the committee. The intent of the CCC is to
ensure all faculty members feel comfortable discussing each resident’s/fellow’s
performance. If the program director is the chair, how comfortable and motivated
are the faculty members expressing their own opinions, versus deferring to the
program director who may “know” many more details about the residents/fellows.
Do the faculty members essentially rubber-stamp the program director’s view? Or
can they provide independent and important judgments necessary to create a valid
consensus, maximizing the strengths of the process, which depend on several,
independent, thoughtful faculty members weighing in?
As with any group process, the program should think strategically about how to
create an atmosphere in the CCC in which all participants feel they can and should
speak candidly and that their opinions will be valued. This committee should be one
of the most important committees in a department and should be known as a place
where faculty members can speak freely and honestly regarding learner
performance in a setting that is supportive, confidential, and structured. Think
intentionally about ways to reduce a hierarchy, perhaps having more junior faculty
members speak first. A faculty chair other than the program director may help
facilitate this process.
In situations where the program director needs to chair the committee, consider
having the program director speak last, after all committee members have provided
meaningful input based on their own observations and experiences. The program
director can be a participant or an observer or not present at all, although many
programs will find it beneficial for the program director to be present to at least
observe and hear the conversations regarding resident/fellow performance.
2. A residency program has 90 residents in a three-year program. The CCC has
its first meeting and can’t imagine faculty members having enough time to
meaningfully review all 90 residents in a practical manner.
There are several options for CCC structure, and since a specific structure is not
dictated by the ACGME, this is an area for programs to be flexible and innovative.
● Some CCCs accomplish this by meeting more frequently—perhaps
three separate meetings at which 30 residents each are considered.
60
● Large programs may have separate CCCs for each PGY cohort (i.e.,
one for the first-years, one for the PGY-2s, and one for the PGY-3s).
Programs using this model may have the individual CCCs follow their
cohort across all years of the program or develop expertise in the
particular curriculum year.
● Some programs may organize their CCCs around specific activities
(e.g., one CCC to assess the QI activities, one for the research
activities, one for ambulatory versus inpatient activities, etc.).
● Some CCCs have organized similarly to an Institutional Review Board,
where one or two members will review a resident’s/fellow’s performance
in detail prior to the meeting and present their assessments and
recommendations to the committee at the meeting, soliciting feedback
from the group.
Programs will gain efficiency by having the CCC think through its expectations of
performance and identify what program assessments best speak to these. When
gaps in assessment tools are identified, it can help the program address them.
CCC members will benefit from faculty development on the Milestones, and on how
best to assess resident/fellow performance. Whatever methods are chosen, the
program coordinator plays a critical role in organizing and providing the right
information to the CCC and its members.
3. A program wants to “democratize” the CCC to reflect resident input by inviting
its chief resident to attend.
Some chiefs are still considered residents, while other chiefs are considered faculty
members. The ACGME precludes a resident (whether or not a chief) from being on
the committee. The rationale is that residents are colleagues of their fellow
residents, and it can be challenging to have them in a situation in which they
engage in high-stakes performance evaluation of these colleagues. The ACGME
allows a chief who has completed a core residency and is eligible for board
certification in his/her specialty to be a CCC member.
Though technically possible to have a faculty-level chief resident as part of the
CCC, the same concern may lead the program to not include such a resident—
they are often just a year away from being a resident themselves and know the
residents very well, and it may be too challenging to engage in the required tasks of
the CCC. On the other hand, input from all residents on their peers is desirable and
may be an important source of data for CCCs, particularly in resident
Professionalism and Communication and Interpersonal Skills milestones. The
program can accomplish this by having regular resident peer feedback as part of its
multi-source/multi-rater evaluation process. Likewise, residents can have a forum to
discuss peer performance and/or send concerns or accolades to the CCC for
review and inclusion in the faculty process.
4. The CCC wants to thoroughly document its process and keep extensive
minutes.
At a minimum, the program director will record the CCC consensus and report
resident/fellow performance on the Milestones to the ACGME. How much of the
61
discussion that informs the Milestones decision is up to the individual program.
Specific, behavioral feedback that would help a resident/fellow improve can be
conveyed as with any program evaluation. This information can be shared with the
resident/fellow as part of his/her twice-yearly evaluation meeting with the program
director, an assigned CCC member, or his/her advisor. The assessment data used
by the CCC to develop its consensus should already be available to
the resident/fellow for review. A written document reflecting the discussion of each
resident’s/fellow’s performance should be:
1. A concise summary of each resident’s/fellow’s performance and any action
or follow-up items
2. Confidential
3. Archived for several years*
*The program should consult with its Human Resources and Legal experts to
understand what should be retained, where it should be archived, and for how long.
5. The CCC and the program director disagree on the Milestone performance of a
particular resident/fellow.
The ACGME Common Program Requirements expect the CCC to provide input, but
the program director to make the final decision on resident/fellow performance
against the specialty-specific Milestones.
6. The CCC wants its faculty members to be more comfortable and candid in their
deliberations, and decides not to share its decision on resident/fellow
performance on the Milestones with the residents themselves.
Residents/fellows should be informed and aware of the Milestones performance
summary the program director is submitting to the ACGME. Currently, the ACGME
does not require programs to have the resident/fellow sign a copy of what is
submitted, but it is considered a best practice. It is required that a copy is
kept in the resident’s/fellow’s performance file. It is expected that programs will
use this as an opportunity to provide feedback to residents/ fellows on their
performance, and to discuss what is needed to get them to the next level. It should
be noted that the ACGME provides individual Milestones data to the
residents/fellows via the Accreditation Data System (ADS).
7. A resident doesn’t agree with the CCC and asks it to change its assessment.
The program director should work with the CCC to clarify and communicate the
program process on options if residents/fellows disagree with the CCC or the
program director’s subsequent assessment of milestone performance. Program
policies and procedures should differentiate the situations in which a resident/fellow
can exercise due process and grievance procedures for an adverse decision. Some
programs would consider the CCC consensus, as a judgement but one devoid of
adverse consequences and would not provide an opportunity for a resident to
“grieve” it. On the other hand, a resident could exercise due process if there were
an adverse program decision (suspension, non-renewal, non-promotion; or
dismissal) based upon the CCC’s Milestones evaluation. Programs should work
62
closely with the DIO and GMEC to ensure program policies are consistent with
institutional policies. HR and Legal contacts may also be useful.
8. The CCC has formed and at its first meeting is deliberating upon the residents’
performance. The Chair is uncertain if they should “call for a vote.”
The authors of this guidebook recommend CCCs not vote. Rather, they
recommend CCCs sufficiently discuss each resident/fellow so they can arrive at a
decision with which each of the members can agree, a true consensus. Calling for a
vote may lead to a situation in which the CCC may appear “divided” and set up a
situation in which its recommendation may be considered uncertain, leaving the
program more vulnerable to a future challenge.

63
Appendix D: Designing the CCC
Completing this table will provide programs with a draft of the required written
description of the CCC, which they can refine and use to educate residents/fellows
and faculty members.
Element
Describe the CCC on this element
Committee Membership
● Appointed by program director
● Minimum of three faculty members
● at least one core faculty member
● Size—“enough,” but all individuals are committed
and able to get to meetings
● Who on the faculty is best able to take on this
role? (i.e., sufficient resident/fellow contact; need
for subspecialty representation)
● Other members? (at the prerogative of and
appointed by program director)
● Physician faculty members from same or other
program(s)
● Health professions with extensive contact and
experience with the program’s residents/fellows in
patient care and other health care settings
● Chief residents who have completed core
program
● Term limits? (five years? the duration of the
residency/fellowship?)
● Staggered appointments? (may be useful to plan
overlap among those joining the committee and
leaving it)
Chair
● Are there requirements/restrictions imposed from
the specialty board or Review Committee
regarding who can chair (or not; e.g.,
anesthesiology program director cannot chair per
American Board of Anesthesiology)?
If no external requirements/restrictions:
● Consider pros and cons of who is best positioned
for this role (goal is to ensure all voices are
heard—if program director chairs, will everyone
simply defer to the program director)
● Program director?
● Associate program director?
● Another faculty member?
● Rotating among members?

64
Element
Describe the CCC on this element
Role/Responsibility of each member
● Where is this information
summarized/documented, and how is it conveyed
to CCC members?
● Confidentiality
● Attempts to mitigate bias
● Meeting attendance
● Term length
● Participation in required professional development
around this role
● Necessary preparation in advance of meeting (is
each member assigned a subset of
residents/fellows to review in advance?)
● Who conveys results to program director (if the
program director is not in attendance at a
meeting)?
Who is responsible for any remediation plan (a
member of CCC, or is this referred to another
individual or group within residency/fellowship?)
Role of the Program Director
● Chair (or not)
● A member
● An observer (perhaps he/she only attends but
refrains from providing input)
● Not present
● Provides feedback from CCC to the
residents/fellows (or not)
Role of Residents/Fellows
● Residents/Fellows are not permitted to be
members of the CCC
● In some programs “chief residents” are faculty
members, and not considered trainees; in this
case it may be appropriate to include them
● Residents/fellows are commonly asked to provide
multi-rater feedback on their peers; this
information is typically used by the CCC as one
assessment of resident/fellow performance on the
Competencies of Interpersonal and
Communication Skills and Professionalism

65
Element
Describe the CCC on this element
(Potential) Role of the Coordinator
Pre-meeting
● Schedule meeting and location
● Notify attendees
● Aggregate data sources (electronically or on
paper)
● Provide information to members before the
meeting so they can engage in any pre-work
● Summarize data, preparing “scorecards” or
“snapshots”
At the meeting
● Provide any information needed by committee
members
● Take minutes
● Document any necessary information to
resident/fellow record
● Record recommendations on each resident/fellow
by milestone
Post-meeting
● Communicate results to program director (if not
present)
● Schedule meetings with residents/fellows and
program director and/or designated faculty
member(s) to review CCC decisions, including
Milestone status
● With program director, submit Milestone
information on each resident/fellow to the ACGME
Shared Mental Model
● How do CCC members develop a shared mental
model of performance?
● What faculty development needs do they have?
● Reaching a common agreement of Milestones
narrative meanings
● Determining how many assessments (and of what
type) are needed for any given milestone
● Determining how to aggregate/interpret data
● Applying QI principles to the evaluation process
● How is this provided? Documented?
● Who is responsible for providing?
● How is any lack of consensus among members
managed?
Consider asking CCC members to self-assess
their performance with specialty-specific
Milestones.

66
Element
Describe the CCC on this element
Meetings
● When?
● Where?
● How frequently? at least twice yearly for most
specialties; could be more frequently, e.g.,
monthly, quarterly
● How long are meetings?
● What is necessary prep to be completed ahead of
meetings, and who contributes to it? What is
deliverable and who is responsible?
How the work of the CCC will be distributed?
● Some CCCs may be responsible for all the
residents/fellows
● Others may be responsible for a subset of the
residents/fellows, (e.g., all PGY-1s, or the
research component of all of the fellows)
● In a large program, there may be CCCs that each
review a specific subset of the residents/fellows
(e.g., three sub-committees of the CCCs each
review 1/3 of the residents/fellows)
Consensus versus Voting
● Preferable to have CCC reach consensus and not
vote
● How are disagreements among CCC members
managed? Documented?
● Program director is the final decision maker
● Guidance from institutional Human
Resources/Legal on how this is
managed/reflected
Integrating assessments from faculty members
external to the program
● If a faculty member not from the program makes
an assessment on resident/fellow performance
with which the CCC disagrees, it is expected that
CCC will take data from evaluations and apply
them to the Milestones to judge the progress of
residents/fellows
● The CCC will have the advantage of knowing how
each of the specialists evaluated the
residents/fellows and can apply that knowledge as
it marks residents’/fellows’ progress on the
Milestones

67
Element
Describe the CCC on this element
Minutes
● What information is captured at the meeting
electronically versus in writing? How is it retained?
● Are there institutional policies that address how
this information is retained (i.e., where? in what
format/for what duration?)?
Measures of Assessment/Tools used by the CCC
● Existing resident assessment data
● What are these?
● How many different types of tools (e.g., multi-rater
feedback, in-service training exam, chart audit of
clinical performance)
● How are these assessments documented?
● How are these assessment shared with
residents/fellows?
● Are there challenges (e.g., faculty members not
completing assessments; milestones for which no
assessment is currently done)? Can the CCC
work with the program to solve these issues?
Measures of Assessment/Tools used by the CCC
(continued)
● Faculty observations
● How are these organized (global end-of-rotation
evaluation, checklist from a procedure, simulation,
standardized patient, miniCEX)?
● How are these documented?
● Used in provision of feedback to
residents/fellows?
● Data from Milestone assessments
● Are these observations captured in such a way
that they provide useful input in Milestone
assessments
Inventory of the Milestones
● Where is each taught in the curriculum?
● How/where/by whom/ is each assessed?
● What are the gaps in teaching and assessment
and what are the plans for addressing them?

68
Element
Describe the CCC on this element
Are there expectations the program has of
residents/fellows that aren’t captured in the
current specialty Milestone(s)?
● How are these communicated to
residents/fellows? To faculty members?
● How are these assessed and documented?
If a resident/fellow is performing sub-optimally:
● Is the CCC (or a member of the CCC) responsible
for an individualized learning plan/ remediation
plan? Another member/group of faculty members?
What are the options for individualized learning/
remediation?
● Intensify mentoring
● Additional readings/structured reading plan
● Skill lab/simulation experiences
● Added rotations
● Repeat rotations/activities
● Extend education
● Counseling to consider another
specialty/profession
Transparency of the CCC process
● How do you describe the CCC process to your
residents/fellows and faculty members (e.g.,
program manual, web page)?
● Is the description of the CCC process up to date
and reflective of actual process?
If a resident/fellow disagrees with a CCC
assessment:
● Review with Human Resources and Legal the
desirability of a grievance process in this
instance (not required by the ACGME)
● Courts (in general) support faculty decisions:
“Made at routine meeting for the purpose of
evaluation”
“Shared understanding of performance”
“Reasonable process”
Residents given notice (of deficiency) and
“opportunity to cure” (ameliorates)
Conscientious decision making
Take into account the entire performance
record

69
Element
Describe the CCC on this element
How do the Milestones fit into promotion criteria?
ACGME Institutional Requirement IV.C.1.:
“The Sponsoring Institution must have a
policy” that requires each of its programs to
determine the criteria for promotion and/or
renewal of appointment…”
How do the Milestones fit into the program’s criteria
for promotion and/or renewal of a resident’s/fellow’s
appointment? Based upon program review:
● Do you need to make any adjustments in your
criteria for promotion and/or non-renewal?
● Do you need to change your agreement of
appointment to reflect Milestone reporting to the
ACGME?
● Do you wish to modify your grievance policy?
o
You may find that you do not need to make any
changes at all, but this is an excellent opportunity
to review your current processes and ensure they
align.

70
Element
Describe the CCC on this element
Using the CCC in continuous educational quality
improvement
● Following the CCC meeting, it may be useful to
debrief
● What types of assessments were particularly
helpful to the CCC in making decisions on
resident/fellow performance?
● Who among the faculty members generated the
most useful assessments (e.g., from explicit,
behaviorally specific narrative comments)
● Do the residents/fellows consistently demonstrate
challenges in their performance on a small subset
of the Milestones? (If so, this may be either a
curricular issue or the lack of an effective
assessment tool)
● What did the program learn from the CCC
experience to help improve the overall educational
and assessment process? (e.g., simplifying the
assessment system; applying examples from the
most useful assessment formats to those that
were least useful)
● What can the program learn from its best
assessors? How can they
acknowledge/reward/use these faculty members
as role models? How can these faculty members’
practices be transferred to other faculty
members?
● Based on this debrief, identify at least one way to
improve assessment in the program
● Specify who will do what, and what exact timeline
to implement the change
● Follow up on results of the improvement at the
next CCC meeting
● Did all faculty members feel able to honestly
represent their views on each resident/fellow?
What impeded/facilitated this ability, and can
enhancements be identified?
Consider making the CCC and its related processes
part of the Annual Program Evaluation
Modified from an earlier table presented by Andolsek, KM and Nagler, A at the
2013 ACGME Annual Educational Conference.

71
APPENDIX E: Examples of Assessment Methods for the ACGME Core
Competencies
Competency
Method
Example
Patient Care
Direct observation
Mini-Clinical Evaluation Exercise;
various apps.
Simulation
Partial task trainers for procedures;
virtual reality
Standardized patient
Objective standardized clinical exams
(OSCEs)
Clinical performance
review
Medical record audits using quality and
safety measures
Procedure log with
assessment of competency
Surgical Case Logs with/without
entrustment scales, potentially with
learner reflection
Faculty evaluations of
observed performance
Evaluation forms using developmental,
supervision, or entrustment scales
Video-captured
performance
Surgical or other procedure; patient
encounter
Virtual reality
Simulation of procedure/ encounter
Multi-source feedback/360-
degree
Feedback from patient experience, team
members, resident/fellow peers
Medical Knowledge
In-training Examination
(ITE)
Most specialties now have an ITE
provided either by their certification
board or a specialty society
Work-based assessments
of medical knowledge
SNAPPS framework; mini-clinical
evaluation exercise (MiniCEX);
Assessment of Reasoning Tool (ART)
Oral-guided chart review
Chart-stimulated recall
Interpersonal and Communication Skills
Multi-source feedback
(MSF)/multi-rater/360-
degree
Some tools available; most home
grown; Teamwork Effectiveness
Assessment Module (TEAM) multi-
source feedback instrument

72
Patient experience surveys
Consumer Assessment of Healthcare
Providers and Systems (CAHPS) suite
of survey tools
www.ahrq.gov/cahps/index.html
Practice-based Learning and Improvement
Self-assessment
Milestones self-assessment followed by
a compare/contrast review of CCC
Milestones ratings with a mentor or
advisor
Evaluation of
resident/fellow teaching
skills
Evaluation forms
Evidence-based practice
(EBP)
Clinical question logs; EBP
prescriptions; EBP assessment of
journal articles
Professionalism
Contribution to institution’s
error reporting process
Spontaneous error reporting; root cause
analysis
MSF/multi-rater/360-
degree
Some tools available; most home grown
Patient survey
CAHPS suite of survey tools
Systems-based Practice
Quality improvement (QI)
project
Can judge the quality of a QI project
using several tools; can measure the
impact of QI project through clinical
performance measures
Contribution to institution’s
error reporting process
Spontaneous error reporting; root cause
analysis

73
Appendix F: Overview of Assessment Methods Aligned with Miller’s Pyramid
(adapted from Lockyer, et al.)
Stage
Corresponding Methods to Assess Performance
Does
Medical record (chart) review
CCC
Direct observation
Efficiency data
End-of-rotation evaluations
Multisource feedback
Patient outcome data
Portfolio
Case Log with assessment
Project review
Shows How
Objective structured clinical exam
Oral case presentation
Simulated case
Skills station
Virtual/computerized patient management
Knows How
Chart-stimulated recall
Development of ILP
Mock oral boards examination
Oral questioning targeting patient management
Written test
Knows
Test (oral or written) targeting fact recall
Reference:
1. Lockyer J, Carraccio C, Chan MK, et al. Core principles of assessment in
competency-based medical education. Med Teach. 2017;39(6):609-616.
https://www.tandfonline.com/doi/abs/10.1080/0142159X.2017.1315082?jour
nalCode=imte20. 2020.

74
Appendix G. PPV (Predictive Probability Value) Tables
PPV tables provide the probability (in percentage terms) that a resident/fellow at
or below a certain Milestone rating (Level) would not achieve Level 4 by time of
graduation. In the example shown below, all PPVs for the Patient Care
Subcompetency (#03) in the Family Medicine Milestones that could be calculated
as of June 2019 are included in the table.
For example, a resident receiving a rating of 2.5 or lower at Milestone review
occasion four, at the end of the PGY-2 has a 54.7% probability (based on national
data) of not achieving Level 4 by the end of the three-year family medicine
residency in this sub-competency.
Example PPV Matrix for the Patient Care Subcompetency (#03) in Family
Medicine: Partners with the patient, family, and community to improve health
through disease prevention and health promotion.
The table shown in this example provides a matrix of all PPVs by Milestone rating
threshold and Milestone review occasions for a single sub-competency for a
single specialty. The tables that follow the box plots in this report for each
specialty provide the PPV matrices for the core specialties and sub-competencies
for which data was available as of June 2019.
PPVs are provided to help identify residents within a program who may be
struggling to match normative national data during each six-month block of the
educational program. This can then be used to support decisions for remediation
or ILPs.

75
Appendix H: ADAPT Model of Feedback
Reference:
1. ADAPT Model of Feedback. University of Washington. Accessible at:
https://depts.washington.edu/lgateway/elearning/feedback/story_html5.html



78
Appendix J: Institutional Checklists for CCCs
(links to institutional oversight of CCCs)
Adapted from Y. Wimberly, MD, Morehouse School of Medicine
✔ Recommended Practices
Comments
for DIO and GMEC
Program incorporates CCC information into APE and identifies
improvements
Regular review of overall resident/fellow milestone performance
and adverse events related to resident/fellow promotion,
program completion, withdrawal, dismissal
Institutional faculty development for CCCs
Program director/core faculty members, and CCC members
participated in program/institutional faculty development for
CCCs, Milestones, and assessment
Quality of CCC documentation across programs (any
expectation this is standardized across programs)
CCCs have “right” membership (> 3 faculty members, including
at least one core faculty member)
Program CCC processes consistent with institutional policies
Sharing of CCC experiences among the institution’s programs
Resident/fellow Milestone performance and/or program CCC
experiences/performance incorporated into Annual Institutional
Review
Program satisfaction with institutional tool(s) such as a resident
management system, used to aggregate performance data for
CCCs
For Program Directors
Need for program “grievance policy” for CCC decisions?
Program director’s CCC role described and acceptable to
specialty
Program faculty development for CCCs
Documented feedback to residents/fellows on their Milestones
performance
Identified enhancements in assessment based on CCC
experiences
CCC Improvements identified as part of Annual Program
Evaluation
Program director has final responsibility for resident/fellow
evaluation/promotion decisions

79
✔ Recommended Practices
Comments
For CCC Chair
CCC conclusions/recommendations are communicated to
program director
Process for how lack of consensus is managed within the CCC
Best practices in group meetings utilized
Review resident evaluations at least semi-annually
For CCC Members
Participate in faculty development (annually?)
Attend specified percent of CCC meetings
Provide requested pre-review of residents and/or meeting
“preparation” prior to meeting
Reach common agreement of Milestone narratives and
understand how assessed
Respect confidentiality
Work to recognize and mitigate biases
For Faculty/Evaluators
Provide timely, honest, high-quality assessments using
appropriate methods to allow CCCs to make informed decisions
regarding resident performance measured against the
Milestones
For Residents/Fellows
Complete Milestones self-assessment before each CCC
meeting?
Compare Milestones self-assessment with program
determination of Milestones assessment following meeting
Co-create an ILP for continued growth with program director or
designee
